
ISMP National Vaccine Errors Reporting Program: 2020-2021 Analysis Focuses on Age-Related, Non-Covid-19 Vaccine Errors
Problem: We recently looked at 1,440 events reported to the ISMP National Vaccine Errors Reporting Program (ISMP VERP) between June 2020 and December 2021. Of note, more than two-thirds (68%) of the vaccine events reported during this timeframe were related to coronavirus disease 2019 (COVID-19) vaccines. We excluded the COVID-19 vaccine events from our analysis since we recently published information about these errors, along with recommended error-prevention strategies (e.g., December 6, 2021; June 30, 2022; July 14, 2022). Our analysis of the remaining reports during the 19-month timeframe showed that the most frequent types of vaccine events, other than those related to the COVID-19 vaccines, were:
-
Wrong vaccine (24%)
-
Expired vaccine or contamination/deterioration (14%)
-
Wrong age (13%)
-
Extra dose (10%)
-
Wrong dose (9%)
-
Vaccine/component omission (e.g., only diluent or a single component of a two-component vaccine administered) (8%)
-
Wrong time or interval (7%)
-
Wrong patient (4%)
-
Wrong route (1%)
-
Other (10%)
Since healthcare providers administer most vaccines in the outpatient setting, reported events occurred in medical clinics (49%), doctors’ offices (20%), public health immunization clinics (11%), or community pharmacies (9%). In these outpatient settings, widespread barcode scanning prior to vaccine administration is often lacking. Only 3% of the events occurred in inpatient settings, and 8% occurred in other settings. Forty-two percent of the events involved registered nurses or nurse practitioners, 34% involved medical assistants, 14% involved pharmacists, and 14% involved other healthcare providers, such as physicians, physician assistants, emergency medical technicians, respiratory therapists, and nursing assistants (more than one practitioner type may have been included in a single report).
Focus on age-related vaccine events
Our focus for this vaccine event analysis is on age-related vaccine errors, which may also be associated with administering the wrong vaccine or the wrong dose. For example, a mix-up between a pediatric hepatitis A vaccine and an adult hepatitis A vaccine could result in an error classified as the wrong vaccine, the wrong dose, or the wrong age. One-third (33%) of the reported events involved the wrong vaccine or the wrong dose, which reporters often attributed to confusion between age-dependent vaccine formulations. Adding these vaccine events to wrong age vaccine events (13%) contributes to nearly half (46%) of all the vaccine errors reported to the ISMP VERP (excluding COVID-19 vaccine errors). Receiving a lower-than-intended vaccine dose for a patient’s age can compromise the protection immunizations provide, leaving patients more vulnerable to diseases; whereas, receiving a higher-than-intended vaccine dose for a patient’s age could result in adverse effects or the need for additional monitoring.
Wrong age and wrong dose events
Wrong age and associated wrong dose errors occurred frequently between age-related formulations of influenza virus vaccines (31%); diphtheria, tetanus, and/or pertussis vaccines, including combination vaccines (23%); hepatitis A vaccines (16%); and hepatitis B vaccines (16%). The frequency of mix-ups between age-related formulations of these four vaccines has not improved much during the past decade. In fact, events related to these four vaccine types seem to be occurring for many of the same reasons previously noted in analyses of the ISMP VERP data between 2012 and 2016, and again in 2017 (June 14, 2018), particularly for:
-
Not differentiating age-dependent formulations of the same vaccine (44%)
-
Failure to verify the patient’s age before administration (16%)
-
Lack of familiarity with the indicated ages for vaccines (16%)
The way vaccine labels portray the intended age group may contribute to some of these mix-ups. It is not surprising that practitioners continue to struggle with providing the correct vaccine based on the patient’s age, given that several vaccines available in pediatric and adult formulations have similar packaging presentations and generic names—some even have the same brand name. Consider three recent vaccine event reports:
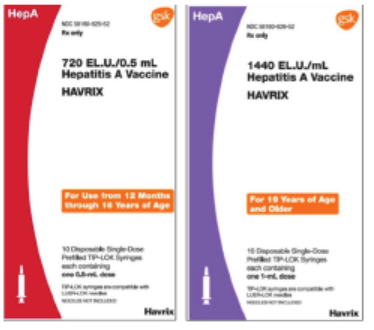
Case 1: A medical assistant administered an adult hepatitis A vaccine (1,440 ELISA units/mL, for patients 19 years and older) to a pediatric patient instead of the pediatric hepatitis A vaccine (720 ELISA units/0.5 mL, for children 12 months through 18 years). A coworker had pulled the adult formulation from the refrigerator, and a medical assistant confirmed what he thought was the correct vaccine and administered it. Both vaccines, manufactured by GSK, have the same brand name, HAVRIX, and the cartons have similar labeling (Figure 1). Although there appears to be plenty of empty space for larger fonts on the carton labels, the print is small and somewhat difficult to read. Also, once a healthcare provider removes a syringe from the carton, the syringe label does not include the recommended age range or specify “pediatric” or “adult” formulation.
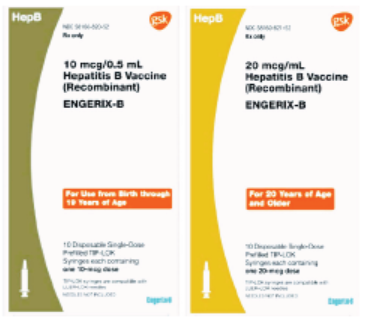
Case 2: A nurse administered the pediatric formulation of hepatitis B vaccine (recombinant), ENGERIX-B (10 mcg/0.5 mL), rather than the adult formulation (20 mcg/mL), to a 28-year-old patient. Both vaccines, manufactured by GSK, have the same brand name, Engerix-B, and the cartons have similar labeling, although the colors used on the left of the cartons are different (Figure 2). Also, the carton labels do not specify “pediatric” or “adult” formulation. Due to a stocking error, the pediatric doses had been stored in the adult bin in the clinic. Prior to administration, the nurse did not check the label, and the outpatient facility did not utilize barcode scanning technology.
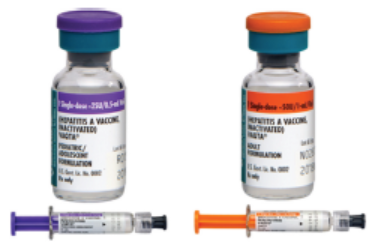
Case 3: A nurse administered an adult hepatitis A vaccine (for patients 19 years and older) to a pediatric patient instead of the pediatric hepatitis A vaccine (for children 12 months through 18 years). The nurse caught the error when documenting the vaccine. Both vaccines, manufactured by Merck, have the same brand name, VAQTA, differing by the color, dose, and pediatric/adolescent or adult formulation designation on the carton, vial, and syringe (Figure 3). However, the indicated age range (pediatric/adolescent or adult) is listed below the vaccine name in similar font size and color, and in all uppercase letters. Practitioners generally identify the vaccine and then stop reading, so they may miss what is below the name and not see “pediatric/adolescent” or “adult.”
Wrong vaccine events
Wrong vaccine events most often involve mix-ups between formulations for different age groups, such as diphtheria, tetanus, and/or pertussis vaccines, including combination vaccines (38%); influenza virus vaccines (17%); meningococcal vaccines (12%); measles, mumps, rubella, and/or varicella vaccines (10%); and hepatitis A vaccines (7%). Underlying causative factors associated with mix-ups among these products included the following:
-
Not differentiating age-dependent formulations of the same vaccine (19%)
-
Look-alike products stored near one another (16%)
-
Similar brand names (15%)
-
Similar vaccine abbreviations (7%)
Consider this recent vaccine event report:
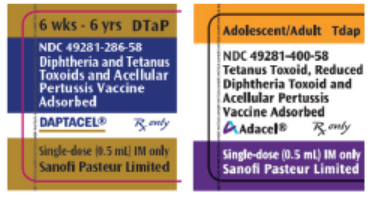
Case 1: A prescriber ordered DTaP (DAPTACEL) to be administered to an infant. A nurse removed the Tdap formulation (ADACEL) from the refrigerator and administered a dose to the infant. Daptacel specifies “6 wks – 6 yrs,” and Adacel specifies “Adolescent/Adult” on the top of the carton (Figure 4). Both products are made by Sanofi and are available in 0.5 mL doses.
Unfortunately, confusion between DTaP and Tdap is among the most common of the age-related mix-ups reported to ISMP. Tdap vaccines contain less diphtheria toxoid and pertussis antigens per dose than DTaP vaccines. These products are easy to confuse due to their similar proper names and abbreviations. The uppercase letters, “D” and “P” in DTaP, correspond with a higher antigen quantity of the diphtheria and pertussis components, relative to Tdap and its lowercase letters. A larger amount of antigen is needed for initial immunization versus a booster shot. An adult who gets DTaP (higher amount of antigens) would not need to be revaccinated but would be more likely to experience adverse effects. But an infant/child who receives Tdap would have received a lesser amount of antigen and may not develop an adequate immune response.
Safe Practice Recommendations: Consider the following recommendations to prevent age-related vaccine errors, help foster herd immunity to prevent disease outbreaks, limit costly overvaccination and re-vaccination, and enhance the public’s confidence in vaccines and the healthcare delivery system:
Maximize technology
-
Develop order sets based on the Centers for Disease Control and Prevention (CDC) immunization schedules to guide prescribers to the appropriate age-based formulations.
-
Along with the full generic name and CDC standard abbreviation, list vaccine brand names in the electronic health record (EHR) and outpatient pharmacy systems, as they may help to differentiate look-alike full vaccine names and combination vaccines.
-
Confirm that clinical decision support will provide an alert if a practitioner orders a vaccine for a patient in an age group outside of its approved indication.
-
Use barcode scanning technology for verification prior to vaccine administration. Expand the use beyond inpatient care areas to offer a greater layer of protection to ensure the patient receives the correct vaccine formulation, as recommended in the 2022-2023 ISMP Targeted Medication Safety Best Practices for Hospitals, Best Practice #18.
Purchase from different manufacturers
-
Investigate purchasing differing age-specific formulations of the same vaccine from different manufacturers to help distinguish them.
Store separately
-
Separate adult and pediatric vaccine storage on different shelves in bins properly labeled with the corresponding age formulation.
-
Do not store vaccines with similar names or abbreviations, or overlapping components (e.g., DTaP, Tdap, TD, Td) right next to each other.
-
For vaccines that come in prefilled syringes, consider storing them in their carton, especially for age-dependent formulations that do not display the intended age range or age group (e.g., pediatric, adult) on the syringe.
-
Assign a staff person to routinely go through the contents of the vaccine bins, opening each carton and making sure no vaccines were incorrectly returned to stock, confirming the intended formulations are still stored separately, and checking that the vaccines have not expired.
Verify identity, age, and vaccine(s) requested
-
When checking in a patient scheduled to receive a vaccine(s), ask the parent, caregiver, or patient to provide at least two patient identifiers—their full name and date of birth. Verify the patient’s actual age with the patient, parent, or caregiver, and ask which vaccine(s) they have requested. Repeat this process immediately prior to vaccination.
-
Ask patients and/or caregivers to bring up-to-date vaccination records/cards to their appointment so they may be reviewed and compared to the EHR.
-
Check your state information immunization system prior to vaccination to ensure the patient requires the intended vaccine.
Label syringes
-
For vaccines that do not come in prefilled syringes, clearly label all prepared syringes (e.g., vaccine name, dose).
-
To facilitate labeling, print patient-specific labels with barcodes or provide practitioners who prepare the vaccines with strips of preprinted labels that differentiate adult or pediatric formulations and doses for each vaccine.
Engage the patient
-
Involve the parent, caregiver, or patient in verifying the vaccine, formulation, and dose by reviewing the label to confirm the correct vaccine. Providing the vaccine information statement (VIS) and reading the medication name and age formulation in the patient’s, parent’s, or caregiver’s preferred language can provide an additional opportunity for both parties to stop and question if something does not seem right.
Document the vaccine(s)
-
Document the lot number and expiration date prior to vaccine administration; this is often the step during which healthcare workers detect an error that can be mitigated. Document administration afterwards in the patient’s profile, on vaccination records, and in state or other immunization information databases.
Educate practitioners
-
When bringing in new vaccine products, including during shortages, educate staff about the new vaccine product, highlighting its storage location, packaging, indication, and the intended age group.
-
In locations where vaccines are prescribed, dispensed, and administered, provide resources that list the indication and schedules for routine and catch-up vaccinations.
-
Use trained providers with demonstrated vaccination competencies to educate staff prior to allowing them to vaccinate patients.
-
Consider focusing on a “vaccine of the month” during staff meetings and/or huddles to draw attention to the vaccine. During this time, review the storage location, packaging, indication, and intended age group, highlighting when there are pediatric and adult formulations. Gather feedback from staff by asking them how this vaccine has caused confusion and led to errors, and make adjustments as needed.
-
Share impactful stories and recognize staff for good catches, describing how the event was averted to prevent future close calls or actual events.
-
Use this document, Staff Educational Topics and Teaching Points to Prevent Errors During Vaccine Administration, as a teaching tool.
Report vaccine-related errors
-
Report vaccine errors internally as well as to the Vaccine Adverse Event Reporting System operated by the US Food and Drug Administration (FDA) and CDC. ISMP also asks providers to report vaccination errors to the ISMP VERP.
Additional resources
-
Please see our past newsletters for additional recommendations to prevent vaccine errors (March 13, 2014; May 22, 2014; March 26, 2015; July 28, 2016; February 23, 2017; June 28, 2018).
Recommendations for FDA and manufacturers
-
We encourage manufacturers to review labeling strategies to reduce the risk of age-related vaccine mix-ups. More can be done by regulators and manufacturers to reduce errors!
-
Prominently display PEDIATRIC or ADULT (or ADOLESCENT/ADULT or PEDIATRIC/ADOLESCENT) formulations in a different color bold font on the top of the cartons, vials, and on syringe labels.
-
For vaccines and other biologics, government regulations require manufacturers to place the product’s proper (generic) name above the brand name. The font size and typeface of the proper name must be at least as prominent as the font size and typeface used in designating the trademark and trade name. However, when reading a label, people generally start from the top, and once they think they have identified the product, they tend to stop reading. Thus, healthcare workers can overlook critical information, including the vaccine’s brand name. While not supported by FDA, for vaccines that have different brand names for vaccine formulations, displaying the brand name prominently and higher on the carton label and vial could help differentiate the various formulations when vaccines have similar generic names.
-
For vaccines that do not come in ready-to-use prefilled syringes, provide pharmacists and vaccine administration staff with preprinted labels (in the carton) that include the vaccine name, dose, and intended age group.
Suggested citation:
Institute for Safe Medication Practices (ISMP). ISMP National Vaccine Errors Reporting Program: 2020-2021 analysis focuses on age-related, non-COVID-19 vaccine errors. ISMP Medication Safety Alert! Acute Care. 2022;27(19):1-5.
Access this Free Resource
You must be logged in to view and download this document.