
ISMP National Vaccine Errors Reporting Program: One in Three Vaccine Errors Associated with Age-Related Factors
Advances in immunization technology and knowledge of diseases have spurred an ongoing stream of new vaccines and periodic changes to vaccination schedules to optimize disease protection. Today, according to the World Health Organization (WHO), immunizations prevent between 2 and 3 million deaths per year. Despite this success, many children and adults in the US remain vulnerable to the 24 vaccine-preventable diseases that are targeted by 45 different single and combination vaccines available today. Some people are vulnerable because they have not been offered vaccinations; others opt-out of recommended immunizations due to misunderstanding. However, errors with vaccines can also leave patients unknowingly unprotected against serious diseases such as hepatitis A and B, pertussis, diphtheria, cervical cancer, and many others.
Since September 2012, ISMP has been operating the ISMP National Vaccine Errors Reporting Program (ISMP VERP) to collect data about the types of vaccine errors and their underlying causes. While it is not possible to determine the frequency of vaccine errors from the ISMP VERP or any other current vaccine error reporting program, given their dependence on spontaneous reporting, estimates from systematic review of vaccination records suggest that errors occur in about 27-35% of all vaccinations.1-3 In this newsletter, we provide a summary of nearly 4 years of vaccine errors reported to the ISMP VERP through June 30, 2016.
Volume and types of error reports
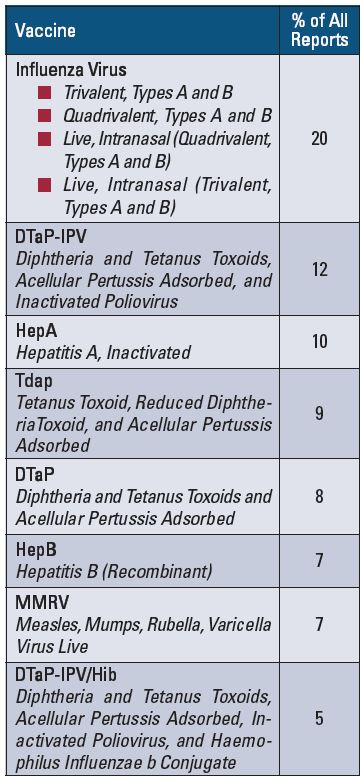
Between September 2012 and June 2016, a total of 1,754 reports have been submitted to the ISMP VERP. Most of these vaccine errors came from practitioners who work in outpatient settings, where most children and adults receive vaccines. Given its voluminous use, influenza virus vaccines were most frequently involved in the reported errors, accounting for 20% of all reports. However, errors involving other vaccines were more common in specific settings based on the typical patient populations served. For example, errors with hepatitis A vaccine were most commonly reported by staff in public health immunization clinics. Errors with zoster and pneumococcal vaccines were frequently reported by staff at community pharmacies. Errors with the anthrax, typhoid, and yellow fever vaccines were most commonly reported by staff at military locations.
The most frequent types of reported vaccine errors included:
- Wrong vaccine (23% of all reports)
- Wrong age for vaccination (20%)
- Wrong vaccine dose (12%)
- Extra vaccine dose (9%)
- Wrong vaccine interval (7%)
The vaccines most often involved in the errors reported to the ISMP VERP can be found in Table 1. The Table also lists the full generic names of the vaccines abbreviated in this report according to the system used by the Advisory Committee on Immunization Practices (ACIP).
Age-related contributing factors in aggregate vaccine reports
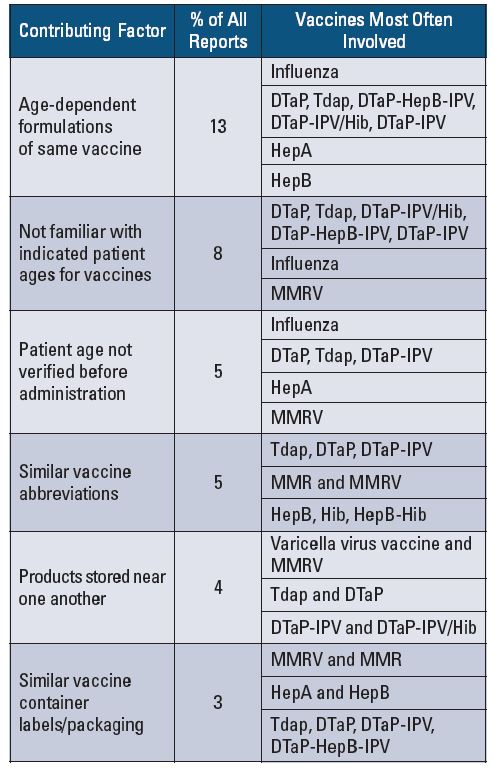
Among all vaccine errors submitted to the ISMP VERP, age-related contributing factors were reported most often and were linked to more than 1 in every 3 error reports (38%) (Table 2). Thirteen percent of all reported vaccine errors were due to confusion that arose between numerous age-dependent vaccines that target the same diseases, particularly with influenza virus vaccines, hepatitis A and B vaccines, and various combination vaccines that target diphtheria, tetanus, and pertussis. Another 13% of the errors involved lack of familiarity with the recommended ages for various vaccines or a failure to take a step as simple as verifying the patient’s age prior to administration. The measles, mumps, rubella, varicella vaccines joined those previously mentioned as one of the most frequently involved in these types of errors. Similar vaccine abbreviations and labeling or packaging, and dense storage conditions, played a role in the remaining 12% of age-related vaccine errors. Along with previously mentioned vaccines, the Haemophilus influenzae type b-containing vaccines were also involved in errors due to labeling or nomenclature problems. We focus this year’s analysis upon these vaccines which were most frequently associated with age-related contributing factors.
Age-related influenza virus vaccine errors
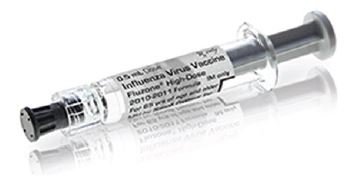
Influenza virus vaccine is available in many formulations that differ based on the patient’s age. The vaccine does not have distinct adult and pediatric formulations. Some formulations are indicated for both children and adults within certain age ranges. Given this and the high frequency of administration in all age groups, it is not surprising that influenza virus vaccine was the most common type of vaccine implicated in age-related errors among vaccines with age-dependent formulations. Many errors involved knowledge deficits regarding the recommended age ranges for each type of influenza virus vaccine and included giving an adult dose/volume of the vaccine to a child or vice versa, administering the high-dose formulation to an adult younger than 65 years, and administering the live nasal formulation to a child younger than 2 years or an adult older than 49 years. Manufacturer labeling and packaging issues that make it difficult to distinguish various age-dependent formulations and US Food and Drug Administration (FDA) requirements to list the generic name before the brand name were also causative factors with many of these errors (Figure 1).
Age-related hepatitis A (HepA) vaccine (HAVRIX, VAQTA) and hepatitis B (HepB) vaccine (ENGERIX-B, RECOMBIVAX HB) errors
Two brands of the hepatitis A vaccine—Havrix (GlaxoSmithKline) and Vaqta (Merck & Co.)—are both available in pediatric/adolescent and adult formulations in 0.5 mL (pediatric/adolescent) and 1 mL (adult) single dose containers. Errors have occurred in which the pediatric/adolescent formulation (0.5 mL) was administered to an adult, and vice versa. These errors were often due to vaccine labeling similarities. While the adult and pediatric/adolescent Vaqta syringes have different color plungers and the vials have different color caps, the text and the primary color on the cartons is similar, and the text on the syringes and vials is small. Color differentiation is also used for the adult and pediatric/adolescent forms of Havrix. However, the syringes must be turned away from the drug name to further view whether it contains an adult or pediatric/adolescent dose. The age notation on vial labels is at the very bottom and is easy to miss.
Similar labeling issues have led to errors with the hepatitis B vaccine. The two vaccines—Engerix-B (GlaxoSmithKline) and Recombivax HB (Merck & Co.)—are available in pediatric/adolescent and adult dose vials and syringes in a consistent concentration but in different volumes. Label differentiation using color has not prevented errors, as the label notations about the different age-based formulations are not prominent. Engerix-B syringe labels must be turned away from the drug name to view the age-specific indication (Figure 2). With Recombivax HB vials, differentiation between the adult and pediatric/adolescent formulations is not prominent (Figure 3) and has led to errors. In fact, one of the most frequently reported events with hepatitis B vaccines involved dosing errors in which a child received an adult’s dose or an adult received a child’s dose.


An additional source of error involves differences in the recommended dosing units of each brand product. For hepatitis A vaccine, the dose is 720 units (0.5 mL) for pediatric/ adolescents and 1,440 units (1 mL) for adults when using Havrix. When using Vaqta, the dose is 25 units (0.5 mL) for pediatric/adolescents and 50 units (1 mL) for adults. Similarly, the recommended doses of the two brands of hepatitis B vaccine are different. Engerix-B dosing is 10 mcg (0.5 mL) for pediatric/adolescents and 20 mcg (1 mL) for adults. Recombivax HB dosing is 5 mcg (0.5 mL) for pediatric/adolescents and 10 mcg (1 mL) for adults. Dosing errors have occurred in which patients received the wrong age-specific volume. In some cases, adults have received half the intended dose when Engerix-B was dosed according to Recombivax HB dosing. One reason the latter errors occurred is that healthcare providers changed from one brand of hepatitis B vaccine to the other without updating the doses or volumes listed in electronic or paper order sets.
Age-related DTaP (DAPTACEL, INFANRIX), Tdap (ADACEL, BOOSTRIX), DTaP-IPV (KINRIX, QUADRACEL), DTaP-HepB-IPV (PEDIARIX), or DTaP-IPV/Hib (PENTACEL) errors
The dominant issues reported with these vaccines are the same issues that have long been reported to ISMP and FDA—confusion between the different age-dependent formulations and combination products. This group of vaccines is particularly vulnerable to errors due to:
- The large number of different vaccines and various combinations of vaccines in this category, many with different targeted ages
- Differences between the recommended ages for the individual components of combination vaccines and the combination vaccine itself
- Similar or confusing manufacturer labeling and/or packaging
- Similarities in standard vaccine abbreviations, the inability to recall the correct abbreviations, and misinterpretation of abbreviations
- The large number of words related to product names to be squeezed into the small space available on single-dose vials or syringes, necessitating a small font size
- Similar generic and brand names
For example, 60 errors have been reported in which DTaP (diphtheria and tetanus toxoids, acellular pertussis) was administered instead of Tdap (tetanus toxoid, reduced diphtheria toxoid, acellular pertussis), or vice versa. Similar vaccine abbreviations and confusion among brand names (Adacel, Boostrix [Tdap]; Daptacel, Infanrix [DTaP]) appear to be contributing factors in these errors, along with not understanding the differences between the two vaccines and the recommended age ranges for administration.
Second only to errors with the influenza virus vaccine, errors with Kinrix (DTaP-IPV) were the most frequent among all vaccine errors. With many of the errors, Kinrix (indicated for children 4 to 6 years old) was given to children younger than 4 years old, when separate components should have been administered to these younger patients. Another common error occurred when Kinrix had been administered instead of the intended vaccine Pediarix (DTaP-HepB-IPV), indicated for children 6 weeks to less than 7 years, or Pentacel (DTaP-IPV/Hib), indicated for children 6 weeks to less than 5 years. Several reports suggest that packaging similarities have led to the mix-ups between Kinrix and Pediarix. More than 50 of the errors with Kinrix also listed staff unfamiliarity with the age-related indications as a contributing factor. Complex vaccination schedules have also contributed to mistakes with the timing of these vaccines, particularly when children are following an alternate or delayed schedule of immunizations.
Most of the age-related errors involving ProQuad were related to administration to children older than 12 years. All but one of the patients were teenagers, and almost half of the errors involved teens who were 13 and 14 years old. Although not mentioned specifically in all these reports, at least some of the errors were associated with teens who were following a catch-up immunization schedule. Once they exceeded the age of 12, the trivalent measles, mumps, rubella vaccine and a separate varicella vaccine should have been administered individually, as the quadrivalent vaccine ProQuad is recommended only for children 12 months to 12 years. Several reporters noted that their electronic health record failed to alert staff that the vaccines were not indicated based on the patient’s age.
Age-related errors with Haemophilus influenzae type b (Hib) components of vaccines
While some errors with Hib or combination vaccines that included the Hib component were related to administration to a patient outside the recommended ages, most were caused by unfamiliarity with the components of combination vaccines or misunderstanding or misreading the HepB component as the Hib component. The latter events led to administration of the Hib vaccine to patients who were not within the recommended age range. For example, numerous reports involved administration of Kinrix (DTaP-IPV) by staff who mistakenly thought it contained Hib, and administration of Pediarix (DTaP-HepB-IPV) instead of Pentacel (DTaP-IPV/Hib), believing the HepB component of Pediarix was Hib.
Safe Practice Recommendations
FDA and vaccine manufacturers, and health professionals who prescribe, dispense, and administer vaccines, are urged to make changes that will reduce the risk of age-related vaccine errors. First, FDA and manufacturers should strongly consider seeking a federal regulatory change that allows the vaccine brand name to be listed first on vaccine labels, before the full generic names, which are often long and confusing. Next, vaccine manufacturers must continue to improve labeling and packaging to differentiate age-dependent formulations of the same vaccine. There are also many practice changes health professionals can make to prevent age-related vaccine errors:
Make safe purchasing decisions
- While not always possible, investigate purchasing different age-specific formulations of the same vaccine from different manufacturers to help distinguish them.
- If possible, stock only one manufacturer’s adult and pediatric/adolescent formulations of the hepatitis A and the hepatitis B vaccines (both adult and pediatric/adolescent formulations from the same manufacturer have the same strength). If both brands must be available in stock, separate their storage, label the storage bins, and, when available, issue electronic reminders to staff to verify the dose.
- Whenever brands change, conduct specific training for all staff and ensure electronic and paper order sets are revised.
Affix warnings
- Affix auxiliary warning labels to vaccines when first received in the clinic, medical office, or pharmacy to draw attention to products with different formulations for neonatal, pediatric, adolescent, and/or adult patients.
- Affix auxiliary labels to select vaccines with problematic similar names to draw attention to key information that would help promote selection of the correct product.
Improve access to information
- Maintain up-to-date easy-to-read electronic immunization schedules for infants, children, teens, and adults, and post them in clinical areas where vaccinations may be administered. Include the brand and generic names of all vaccines, the approved abbreviations, and the range of ages appropriate for administration. (We could not find a list of all brand and generic vaccines and their age-specific recommendations, but adding this information to the current list of vaccines and acronyms provided by the ACIP would be very useful.)
- On order sets, medication administration records (MARs), and vaccination records, list the brand names and all components of combination vaccines. When space permits, list full generic names of all components. If abbreviations must be used, employ only the ACIP approved abbreviations (see link above). Make necessary revisions if brands change.
Store vaccines safely
- Store vaccines in refrigeration and freezer units large enough for organized and labeled stock.
- Separate pediatric and adult formulations of vaccines in storage areas.
- Label the specific locations where vaccines are stored to facilitate correct, age-specific selection (Figure 4).
- Do not store vaccines with similar labels, names, abbreviations, or overlapping components (e.g., DTaP, Tdap) immediately next to each other.
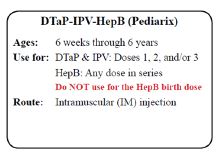
Figure 4. Example of label for storage locations of vaccines.
Educate patients and caregivers
- Provide all patients, parents, or legal guardians with a Vaccine Information Statement (VIS) in their preferred language prior to vaccination. If a combination vaccine contains the components DTaP, HepB, Hib, or IPV, provide the Pediatric Multiple Vaccine VIS. VISs are available on the Centers for Disease Control and Prevention (CDC) and the Immunization Action Coalition websites and have been translated into more than 40 languages. The VISs can be printed, viewed, and displayed on smart phones, tablets, or other mobile devices and imported into an electronic file. Time to read the VIS and ask questions before vaccination should be provided.
Verify the patient’s age
- Prior to prescribing, dispensing, or administering a vaccine, verify the patient’s age by asking the patient or caregiver for a birth date and referencing the patient’s health record, immunization record, and/or MAR. Also check immunization registries before ordering and administering vaccines to verify the patient’s current vaccination status and indicated ages for administration.
- Prior to vaccine administration, compare the patient’s current age with information on an applicable immunization schedule and VIS.
- Ask patients or parents to help verify the vaccine prior to administration by reading the VIS and checking that the patient is within the specific ages for the vaccine.
- Employ point-of-care barcode scanning to verify that the correct vaccine and age-specific formulation has been selected and prepared for administration to a patient.
- Build alerts in order entry systems to warn health professionals if a specific vaccine is prescribed and selected for a patient who is older or younger than the recommended ages for vaccine administration.
Educate staff
- Discuss vaccine errors that can occur and how to prevent them with health professionals who prescribe, dispense, and administer vaccines.
References
- Lang S, Ford KJ, John T, Pollard AJ, McCarthy ND. Immunisation errors reported to a vaccine advice service: Intelligence to improve practice. Qual Prim Care. 2014;22(3):139-46.
- Feikama SM, Klevens RM, Washington ML, Barker L. Extraimmunization among US children. JAMA. 2000;283(10):1311–7.
- Butte AJ, Shaw JS, Bernstein H. Strict interpretation of vaccination guidelines with computerized algorithms and improper timing of administered doses. Pediatr Infect Dis J. 2001;20(6):561–5.