
Three New Best Practices in the 2024-2025 Targeted Medication Safety Best Practices for Hospitals
ISMP has released its 2024-2025 Targeted Medication Safety Best Practices for Hospitals, whose purpose is to identify, inspire, and mobilize widespread, national adoption of consensus-based Best Practices to address recurring problems that continue to cause fatal and harmful errors despite repeated warnings in ISMP publications. The Best Practices, which are reviewed by an external expert advisory panel and approved by the ISMP Board of Directors, represent high-leverage error-reduction strategies, many of which have already been successfully adopted by hospitals. While the Best Practices might be challenging for some organizations to achieve, they are all practical and realistic, and their value in reducing medication errors is grounded in scientific research and/or expert analysis of medication errors and their causes. Their implementation can vastly improve medication safety and reduce the risk of significant patient harm. While these Best Practices were created for hospitals, some are applicable to other healthcare settings. ISMP also offers a version for community pharmacy.
New Best Practices for 2024-2025
Initially introduced in 2014 with six Best Practices, the Targeted Medication Safety Best Practices for Hospitals are updated every 2 years. The 2024-2025 list now comprises 22 Best Practices, including three new Best Practices described below.
New Best Practice 20: Safeguard against wrong-route errors with tranexamic acid.
- Utilize point-of-care barcode-assisted medication safety checks prior to administering medications in surgical and obstetrical areas.
- When appropriate, use premixed intravenous (IV) bags of tranexamic acid, which are less likely to result in mix-ups than vials of tranexamic acid.
- If possible, do not store tranexamic acid in an anesthesia tray.
- Separate or sequester tranexamic acid in storage locations (e.g., pharmacy, clinical areas) and avoid storing local anesthetics and tranexamic acid near one another.
- To prevent misidentifying medications by viewing only the vial caps, avoid storing injectable medication vials in an upright position, especially when stored in a bin or drawer below eye level. Store them in a way that always keeps their labels visible.
- Conduct a review to identify any look-alike ampules or vials (including caps) and determine if the risk of a mix-up will be reduced by purchasing them from different manufacturers. If so, purchase them from different manufacturers.
- Consider labeling vial caps with a label that states, “Contains Tranexamic Acid.”
New Best Practice 21: Implement strategies to prevent medication errors at transitions in the continuum of care.
- Obtain the most accurate medication list possible upon admission to the organization before the first dose of medication is administered (except in emergency or urgent situations).
- Include asking about allergies and associated reactions, prescription, and over-the-counter medications (including herbals and dietary supplements), and non-enteral medications.
- List the drug name, dose, route, frequency, indication, and time of last dose.
- Consider assigning dedicated practitioners to obtain medication histories.
- Ensure the medication and doses collected and subsequently ordered are correct therapy for that patient, given their current state of health.
- Designate a provider to compare the prescribed medications to those on the medication history list and resolve any discrepancies. Have providers document reconciliation and modifications made to current therapy upon admission, with each change in level of care, and at discharge.
New Best Practice 22: Safeguard against errors with vaccines administered in the inpatient and associated outpatient settings.
- Utilize standard order sets to prescribe vaccines. Require an order prior to administration of any vaccine. Utilize the full generic name and brand name (if applicable) and avoid vaccine abbreviations.
- Verify a patient’s immunization status (in the electronic health record [EHR] as well as vaccine registries) prior to providing vaccines.
- Provide patients and/or caregivers with vaccine information (e.g., Vaccine Information Statement [VIS]) in their primary language prior to vaccination.
- Store vaccines in separate bins or containers based on type and formulation. Store two-component vaccines together.
- Use prefilled syringes when available. If not available, prepare each vaccine dose immediately prior to administration and label with the vaccine name, dose, and if appropriate, the indicated age range.
- If multiple adults and children are being vaccinated at the same time, separate them into distinct treatment areas; bring only one patient’s vaccines into the treatment area at a time.
- Verify the patient’s identity using two unique identifiers.
- Use barcode scanning technology to verify the correct vaccine and dose are being administered to the correct patient.
- Document the vaccine’s national drug code (NDC) number, lot number, and expiration date prior to administration; document administration in the EHR, and ensure information is sent to the local or state vaccine registry.
- Provide vaccinators with ongoing education and competency assessment about vaccines and their appropriate storage, selection, administration, and monitoring.
Additional Changes for 2024-2025
Where additional information and/or changes were made to other Best Practices, the addition/modification is italicized in the specific Best Practice listed below (refer to the full document to review the complete Best Practice statements):
Best Practice 7: Segregate, sequester, and differentiate all neuromuscular blocking agents (NMBs) from other medications, wherever they are stored in the organization.
- Eliminate the storage of NMBs in areas of your organization where they are not routinely needed.
- Limit availability in automated dispensing cabinets (ADCs) to areas where they are needed such as perioperative, labor and delivery, critical care, and emergency department (ED) settings; in these areas, store them in a rapid sequence intubation (RSI) kit or locked-lidded ADC pockets/drawers.
- Place auxiliary labels on all storage bins (both refrigerated and non-refrigerated) and/or ADC pockets and drawers that contain NMBs.
- Configure interactive ADC alerts that require users to enter or select clinically relevant information (e.g., the purpose for removing the drug [a code situation], whether the patient is ventilated) prior to removal.
Best Practice 8: Administer all* medication and hydration infusions via a programmable infusion pump utilizing dose error-reduction systems.
*Unless the rate of the infusion exceeds the delivery limits of the infusion pump.
- Further, implement bi-directional (e.g., auto-programming and auto-documentation) smart infusion pump interoperability with the electronic health record and establish organizational expectations (e.g., compliance goals) for the use of auto-programming and documentation for medication and hydration infusions.
Best Practice 11: When compounding sterile preparations, utilize workflow management systems.
- Minimize sterile compounding outside of a pharmacy environment.
- Follow safe pharmacy processes for use of technology.*
- Identify safety gaps specific to each technology and create an action plan to avoid errors.
- If you are not currently using workflow management systems, create an implementation plan.
- Before implementing compounding technology, perform a failure mode and effects analysis of the new system and workflow process.
*See ISMP Guidelines for Sterile Compounding and the Safe Use of Sterile Compounding Technology
Best Practice 15: Verify and document a patient’s opioid status (naïve versus tolerant*) and type of pain (acute versus chronic) before prescribing and dispensing extended-release and long-acting opioids.
*Adult opioid-tolerant patient: Opioid tolerance is defined by the following markers: Patients receiving, for 1 week or longer, at least: 60 mg oral morphine/day; 25 mcg transdermal fentaNYL/hour; 30 mg oral oxyCODONE/day; 8 mg oral HYDROmorphone/day; 25 mg oral oxyMORphone/day; 60 mg oral HYDROcodone/day; or an equianalgesic dose of another opioid, including heroin and/or non-prescribed opioids.
Best Practice 17: Safeguard against errors with oxytocin use.
- Require the use of standard order sets for prescribing oxytocin antepartum and postpartum that reflect a standard clinical approach in your organization for labor induction/augmentation and to control postpartum bleeding.
- Standardize to a single concentration and bag size for both antepartum and postpartum oxytocin infusions (e.g., 30 units of oxytocin in 500 mL of Lactated Ringer’s solution).
- Communicate orders for oxytocin infusions in terms of the dose rate (e.g., dosage/time) and not by the volume rate (e.g., volume/time) and align with the smart infusion pump dose error-reduction system (DERS).
- Provide oxytocin in a standard ready-to-administer form.
Best Practice 19: Layer numerous strategies throughout the medication-use process to improve safety with high-alert medications.
- Engage patients and family members to improve safe use of high-alert medications by providing targeted education to those receiving select, defined high-alert medications.
- Include strategies to address health equity and literacy issues.
- Establish criteria to trigger an automatic consultation with a pharmacist or patient educator, diabetes educator, social services, or home care. Specific drugs to consider for targeted education: insulin, U-500 insulin, methotrexate, oral (and injectable) chemotherapy, opioids, investigational medications, anticoagulants, any medication that has an administration device (inhalers, pens, ambulatory infusion pumps), medications that require dose sequencing or ‘titration.’
Prior Survey Results
Between February and March 2022, ISMP conducted a brief survey to obtain a baseline measurement of the three new Best Practices added in the 2022-2023 edition. Prior to releasing the 2024-2025 Targeted Medication Safety Best Practices for Hospitals, ISMP conducted an additional survey between May and June 2023 to measure the progress with implementing the existing 2022-2023 Best Practices. These results were presented at the American Society of Health-System Pharmacists (ASHP) Midyear Clinical Meeting on December 5, 2023. An overview of the survey findings is provided in Table 1.
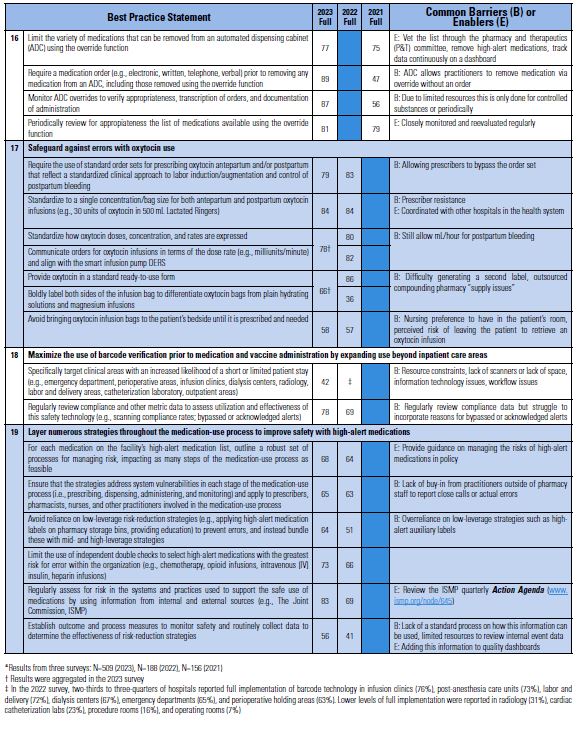
Table 1. Percentage of respondents reporting full implementation of the 2022-2023 Targeted Medication Safety Best Practices for Hospitals* compared to previous years (2022 and 2021).
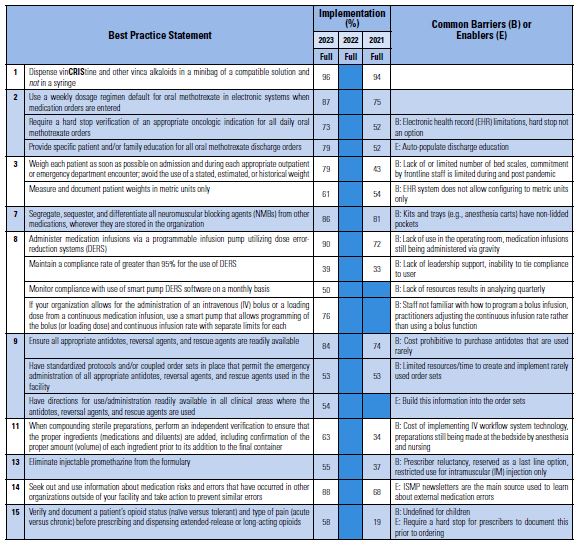
More than five hundred (n=509) respondents participated in our 2023 Best Practices survey. Almost one-tenth (9%) of the hospitals that participated indicated they have 500 beds or more; 11% have 300-499 beds; 38% have 100-299 beds; 30% have 26-99 beds; and 12% have 25 beds or less. Overall, 87% of responding hospitals reported having one or more part- or full-time medication safety officer(s) (MSO).
Comparing the 2023 survey findings to previous survey findings in 2022 and 2021, the number of respondents reporting full compliance with the Best Practices increased for nearly all items. Of note, regarding Best Practice 17, safeguard against errors with oxytocin use, in 2022 86% of hospitals reported full implementation regarding provision of oxytocin in a ready-to-use form and around one-third (36%) responded that they boldly label both sides of the infusion bag to differentiate oxytocin bags from plain hydrating solutions and magnesium infusions. This question and results were aggregated in the 2023 survey, with 66% reporting full implementation of both components.
We were pleased to see that several of the Best Practices had large upsurges in hospitals reporting full implementation. This included components from Best Practice 2 (require a hard stop verification [or clarification if a hard stop is not possible] of an appropriate indication for daily methotrexate orders, and provide education to patients discharged on oral methotrexate), Best Practice 3 (weigh patients as soon as possible on admission/encounter), Best Practice 11 (independently verify the ingredients and amount/volume prior to adding them to compounded sterile preparation containers), Best Practice 15 (verify/document a patient’s opioid status and pain type before prescribing/dispensing extended-release or long-acting opioids), and Best Practice 16 (require a medication order prior to removing any medication from an ADC including those removed via override, and monitor ADC overrides to verify appropriateness).
Conclusion
Hospitals and health systems should focus their medication safety efforts over the next 2 years on these new and any not fully implemented 2024-2025 Best Practices. The rationale for recommending the Best Practices, along with related ISMP publications and guidelines for additional information, can be found in the full document. Related documents that might be helpful to hospitals include Frequently Asked Questions (FAQs) and an Implementation Worksheet to help hospitals identify gaps in the implementation of these Best Practices and develop an action plan to address vulnerabilities.
Survey to Measure Baseline Implementation of New Best Practices
ISMP is conducting a brief survey to obtain a baseline measurement of the current level of implementation of the new Best Practice statements. We would sincerely appreciate your participation in this survey, regardless of whether you have implemented any of the Best Practices. Please complete the online survey by April 19, 2024, by clicking here.
Suggested citation:
Institute for Safe Medication Practices (ISMP). Three new best practices in the 2024-2025 targeted medication safety best practices for hospitals. ISMP Medication Safety Alert! Acute Care. 2024;29(4):1-6.
Access this Free Resource
You must be logged in to view and download this document.