
Survey Shows Recession Has Weakened Patient Safety Net
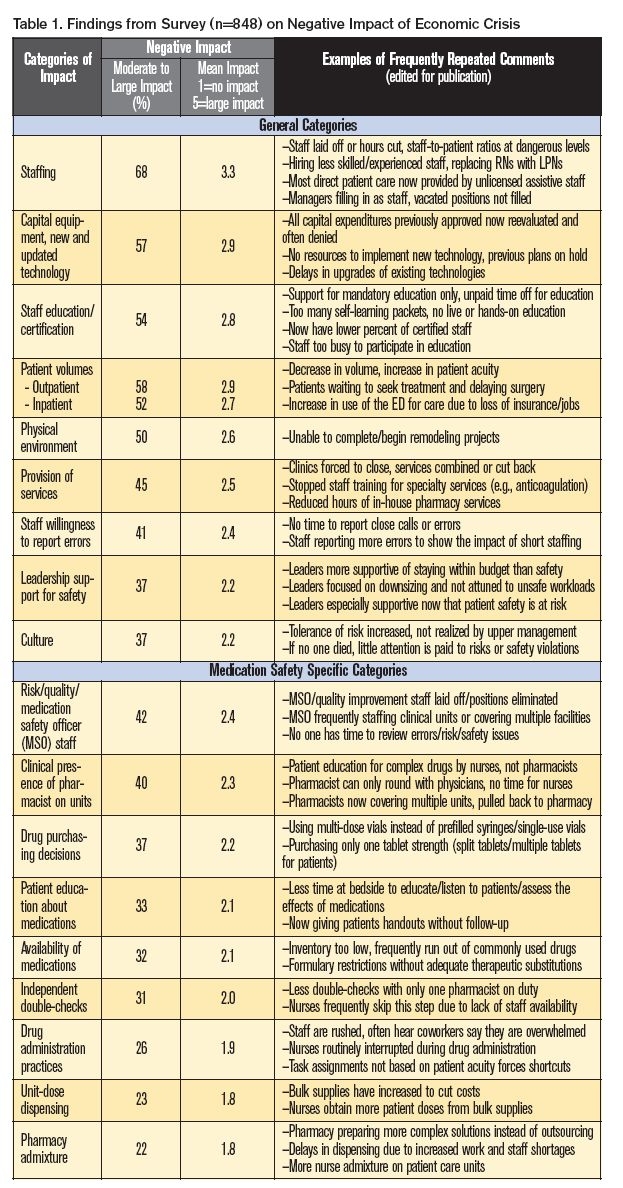
As we listen to the news, it is clear that the current recession has impacted nearly every sector of the economy. According to 848 respondents to a survey we conducted in September through November 2009, healthcare is likely no exception. Our survey findings support conclusions drawn from an earlier 2009 survey by the American Hospital Association1 (AHA), which found that the economy has taken a toll on the patients and communities that hospitals serve. In addition to the financial woes that make it difficult to conduct business, hospitals are facing a second threat—the increased risks to the patients they serve, stemming from the steps many hospitals may be forced to take to respond to the economic downturn.2 Although our survey methodology does not meet the rigors of scientific research, our results offer a glimpse of the impact these steps are having on both healthcare staff and patient safety, including the impact on medication safety. (Table 1)
Respondents to our survey were predominantly nurses (75%) and pharmacists (16%) working at a staff (51%) or managerial/director level (28%) in hospitals (87%). It was clear from respondents that the survey touched upon a worrisome topic, generating thousands of additional comments (see Table 1) covering more than 70 pages of printed text. Nearly one-quarter (20%) of respondents reported a large negative impact on medication safety in their hospitals due to the economy; another 21% reported a moderate negative impact. Similar results were found regarding the impact on patient safety in general.
General Patient Safety Findings
More than two-thirds of respondents reported that the economy has affected their staffing. Survey comments suggest that layoffs, staff attrition without replacement, hiring less experienced staff, and reductions in salary/paid vacation have occurred widely, and that remaining staff often fear losing their jobs, particularly if leaders do not share information about how the organization plans to deal with the economic impact. About the same percent of respondents reported that the economy was taking a toll on staff morale, often citing unsafe workloads due to staff reductions and the inability to provide quality and safe care as key contributing factors.
Half of the survey respondents felt that the economy has adversely impacted the purchase of capital equipment, implementation of technology, updating of existing technology, and remodeling of the physical environment. Plans have been placed on hold, and all expenditures—even those previously approved—are being reevaluated. Half of the respondents also reported that the economy is affecting their ability to participate in external and in-house education. Some respondents reported an overall reduction in certified staff; many stated they were too busy to attend educational programs and/or their organizations were no longer able to provide financial support for such programs. Reductions in staff, educational opportunities, capital expenditures, and remodeling were also linked to a reduction in the provision of new and/or existing services, such as ambulatory care clinics, anticoagulation services, and 24-hour pharmacy services.
At least half of the respondents reported that the struggling economy has also impacted the patient census, citing a decrease in inpatient and outpatient volumes but an increase in patient acuity. Many respondents felt that patients are delaying surgery and medical treatment, thereby increasing their acuity when they present for treatment. Numerous respondents also reported a corresponding increase in emergency department (ED) visits, particularly for patients without insurance—a finding substantiated in the recent AHA survey of hospital chief executives.1
According to respondents, the organizational culture, staff willingness to report errors, and leadership support for safety have been the least impacted by the economy. Still, a third of the respondents reported a decidedly negative effect from the economy on these elements of a culture of safety. Lack of time to report close calls was the most common response in the survey, followed by staffs’ tolerance to risk, which may not be acknowledged by organizational leaders. However, a few respondents told us that staff are now reporting more close calls and errors in an attempt to keep administration informed about new risks associated with staff reductions and other cost-cutting measures. Like-wise, a few respondents reported that their leaders are especially supportive of patient safety now because they recognize the risks to patients during this economic crisis.
Medication Safety
Half of respondents reported that the economy has forced a reduction in dedicated time or the total elimination of a medication safety officer (MSO) position or quality/risk management staff dedicated to medication safety. If the MSO/quality/risk management positions were not eliminated, respondents noted that these practitioners were often asked to staff clinical units, when needed. Some respondents told us that the prior MSO’s responsibilities were assumed by others (e.g., chief nursing officer, director of pharmacy); however, in reality, time did not permit these staff to properly receive, review, analyze, and implement changes for problems associated with medication safety.
One-third of respondents reported that economic conditions have resulted in less safe drug purchasing decisions, such as switching to multiple-dose vials instead of using single-use vials and prefilled syringes. One-third of respondents also reported reduced availability of medications because their organizations had decreased inventory due to the economy. Many respondents who provided comments noted that they had even run out of frequently prescribed medications during the past year. A few suggested that new formulary restrictions have made important drugs unavailable without adequate therapeutic equivalents or substitutions.
More than one-third of respondents told us the clinical presence of pharmacists on patient care units has been impacted by the economy. Most often, respondents commented that clinical pharmacists were pulled back into the pharmacy for drug distribution duties or required to cover more patients/units/facilities. Some nurses noted that, when clinical pharmacists are on the unit, they now only have time to round with physicians or do computer work, making them less available to nurses than they were previously. One-third of respondents reported less time and staff to educate patients about medications and to conduct independent double-checks of high-alert medications before they are dispensed or administered.
One-quarter of nurse respondents reported that staff reductions due to the faltering economy have led to hurried drug administration practices during which shortcuts are sometimes taken to get the work done. Likewise, about one-quarter of pharmacy respondents reported an increase in delays in dispensing pharmacy-prepared parenteral products and solutions, or nurses mixing more products on patient care units. Some respondents also commented that fewer admixtures are now being outsourced to external companies, which has also resulted in dispensing delays. Similarly, fewer products are being dispensed in unit doses.
Conclusions
According to respondents, the faltering economy may be causing an adverse effect on patient safety in a number of hospitals, although not all. The true risk to patients is yet to be determined. About 20% of respondents reported that medication errors have occurred in the past year in which changes due to the economic downturn were a contributing factor. Many error descriptions provided by respondents included mistakes with high-alert medications, such as insulin, narcotics, neonatal electrolyte solutions, heparin, low molecular weight heparin, and chemotherapy. Perhaps these errors were the most memorable to respondents since the risk of patient harm from errors with these drugs are so great. Although no patient deaths were reported to us through the survey, we fear that these survey findings are a harbinger of things to come.
Some economists predict that the adverse effects from the economy will come later in healthcare than to other business sectors.2 For those in healthcare who already feel the pinch, the worst may be yet to come as employers and third-party payers continue to tighten reimbursements and patients continue to experience financial burdens that lead them to delay seeking medical care until their health worsens. One thing is clear. Healthcare is likely not immune from the effects of the faltering economy. Only 27% of our respondents reported that leaders in their organization have developed a plan to minimize the backslide on patient safety during the economic downturn. We encourage all healthcare organizations to plan for the inevitable effects of the economy with a steadfast goal to maintain patient safety.
References
- American Hospital Association (AHA). The economic crisis: the toll on the patients and communities hospitals serve. April 27, 2009.
- AHC Media. Downturn in economy may bring more challenges for risk managers. Healthcare Risk Management March 2009;31(3):25-28.