
Oops, Sorry, Wrong Patient! A Patient Verification Process Is Needed Everywhere, Not Just at the Bedside
Problem: When you think of “wrong patient” medication errors in inpatient settings, the most common scenario that comes to mind is a nurse walking into a patient’s room and administering medications intended for one patient to another patient—often a roommate. Perhaps the patient had switched hospital beds with his roommate to be closer to the window, or he was sitting on the edge of his roommate’s empty bed. Maybe the nurse had verified the patient’s identity during initial drug administration but failed to check it again during subsequent administrations that day.1 Or the process of verifying the patient’s identity was interrupted by a visitor asking a question, and the nurse simply forgot to complete the verification process. In any case, one fundamental cause of these errors is a flawed or absent patient identification process.
However, “wrong patient” medication errors can occur for a variety of reasons at any point in the patient encounter or during any phase of the medication use process. Examples of hazards, near misses, and actual “wrong patient” errors follow. Fictitious names are provided when necessary to convey the basis of the error.
Patient Registration
Omitting junior/senior designation. A patient’s son, John Jones Jr., was registering to donate stem cells for his father, John Jones Sr.1 After confirming the son had previously been a patient in the hospital, the registration clerk located “John Jones” in the master patient list, printed an armband, and placed the armband on his wrist. The clerk was focused on the technical aspects of entering data, and little attention was given to verifying the patient’s identity before applying the armband. A clerk later realized that both father and son were wearing identical armbands. Thus, any medications prescribed for the father could have been administered to the son, or vice versa, even if the nurse had properly identified the patients using name and medical record number.
Prescribing
Order entry error. A dehydrated lung cancer patient was admitted to the emergency department for IV hydration. Another patient from a motor vehicle accident (MVA) was awaiting intubation and transfer to a local trauma center. The same physician was caring for both patients. The physician gave verbal orders for vecuronium and midazolam for the MVA patient, but he inadvertently entered the medication orders electronically into the cancer patient’s record. The nurse caring for the cancer patient went on break, and a covering nurse administered the paralytic and sedative to the cancer patient even though he was not intubated. The patient experienced a respiratory arrest and died.
Reliance on wrong patient data. A physician prescribed medications for a new patient that were based on a medication list in the history and physical of the patient’s sister. A pharmacist discovered the error during medication reconciliation.
Transcription
Mistranscribed telephone order. A nurse accepted a telephone order for morphine 2 mg IV but transcribed the order onto the wrong patient’s record. The order was faxed to the pharmacy and entered as an active order on the wrong patient’s electronic medication administration record (eMAR). The wrong patient, who was already receiving fentaNYL, was given the morphine, which caused significant respiratory depression. A rapid response team was called, and naloxone was administered.
Intermingled patient labels. When a consulting physician arrived on a unit to follow-up with a known patient, he learned the patient and chart were both in radiology. The physician wrote several orders on a blank order form and asked the unit secretary to add a patient label. The labels for all active patients were kept together in a single file folder. The unit secretary located labels for the correct patient but accidentally removed a label from another patient’s supplies that were right behind the correct labels. The incorrect label was affixed to the order form. The error was captured before reaching the wrong patient.
Dispensing
Data entry errors. To enter an order for a patient named Franklin Hope, a pharmacist tried to access the profile using the patient’s identification number. However, the number was poorly visible on the order form imprint, and the profile could not be located. He then entered the patient’s name, Franklin Hope, and a profile appeared on the screen. While entering the order, the pharmacist happened to notice that the patient was female, not male. He soon realized that he had been entering the order into Hope Franklin’s profile, not Franklin Hope’s profile!
Coupled drug delivery. An oncology patient received another patient’s IV chemotherapy despite patient verification by two nurses before administration. Typically, the pharmacy dispensed each patient’s chemo-therapy inside a labeled Ziplock bag. In this case, the pharmacy sent chemotherapy for two patients inside the same Ziplock bag. When the contents of the bag were removed, the nurses discovered there were chemotherapy bags for two patients. They verified the first patient and the chemotherapy for that patient, but the nurse administering the chemotherapy accidentally picked up the other patient’s chemotherapy bag and administered it to the first patient.
Administration
Reliance on verbal affirmation of name. A nurse entered the waiting area of an oncologist’s office and called for “Mrs. Jackson” to come back to the treatment room for her chemotherapy.1 The nurse carefully checked the chemotherapy orders against the medical record the receptionist had handed her. Verifying only that the patient was Mrs. Jackson, the nurse prepared and administered the chemotherapy. Several hours later, another patient named “Mrs. Jackson” arrived for chemotherapy, and the nurse realized she had administered this patient’s chemotherapy to the prior patient named “Mrs. Jackson.”
ADC overrides entered into eMARs. In two instances, the wrong patient was selected from a patient list on the screen of an automated dispensing cabinet (ADC) in a cardiac catheterization (cath) lab. The ADC allowed access to all patients in the hospital. This ADC could be configured to limit access to patients on up to six units. However, the cath lab needed access to patients in more than six units, so it was configured to allow access to all hospitalized patients. When withdrawing medications from the ADC in the cath lab, the search for the correct patient was typically narrowed by entering the first part of the patient’s account number or last name, and then picking the correct name among the list that appeared on the screen. In the two events, nurses incorrectly picked the names of infants in the NICU instead of similarly named adult patients who were scheduled for cardiac catheterizations. When the medications were removed from the ADC under the infants’ names, it created an override that populated the drugs on the infants’ eMARs. Fortunately, the erroneous entries in the eMARs were noticed before the infants received the drugs prescribed for the adult cardiac cath patients.
Mixing up MARs. The medication administration records (MARs) for two infants were mixed up, resulting in the administration of SYNAGIS (palivizumab), used to protect infants/young children from respiratory syncytial virus, to the wrong child. The infants were side-by-side in isolettes, and both MARs were on the counter between the two isolettes. Coincidentally, both infants had the same first name along with very similar hospital identification numbers. The nurse failed to notice that she was referring to the wrong MAR and administered a dose of Synagis to the wrong infant.
Monitoring
Mixing up monitoring results. A physician prescribed CARDIZEM (diltiazem) 20 mg IV followed by 30 mg orally for a patient in bed A after a telemetry unit nurse called to report that his cardiac monitor showed atrial fibrillation and flutter with a heart rate of 140. When the patient exhibited no improvement after receiving the drug, the nurse called the physician again and received an order to administer 150 mg of amiodarone IV push followed by a 60 mg per hour infusion. A short time later, the nurse realized that the rhythm she was viewing on the monitor at the nurse’s station was for the patient in bed B. The names of the patients in bed A and bed B had been mixed up and posted on the wrong channel of the central monitoring unit.
Safe Practice Recommendations
First introduced in 2003, The Joint Commission National Patient Safety Goal (NPSG) #1 aims to improve the accuracy of patient identification. Today, the goal requires healthcare practitioners to use at least two patient identifiers (not the patient’s room number or location) when providing care, treatment, and services. The intent is two-fold: 1) to reliably identify the individual as the person for whom the service or treatment is intended, and 2) to match the service or treatment to that individual.
The 2011 Elements of Performance for this goal require healthcare workers to verify patient identity using at least two identifiers when administering medications, blood, and blood components; when collecting blood samples and other specimens for clinical testing; and when providing treatments or procedures. Lest you believe that only tasks associated with drug administration are included, The Joint Commission has noted in questions and answers on this goal that it applies to “other treatments and procedures,” including, for example, prescriber’s orders and reporting of test results.
Thus, patient verification using two identifiers should be accomplished with all patient-associated tasks in the medication use process when:
- Physicians prescribe medications
- Pharmacists and technicians enter/verify orders and dispense medications
- Unit secretaries, nurses, and other authorized staff transcribe medication orders
- Nurses and other qualified healthcare providers administer medications
- Healthcare workers set up, obtain, receive, give, and/or document/file diagnostic test results (which are often relied upon for medication prescribing)
- Healthcare practitioners participate in other critical processes.
Nurses should have the patient’s MAR or eMAR at the bedside for verification of two unique identifiers. Pharmacists and pharmacy technicians who enter orders into the pharmacy computer should select the patient profile using the patient’s medical record number (never the room number) or by scanning the barcode on the patient’s label on an order set, and then confirm the patient’s name and number on the screen by comparing them to the name and number on the orders; unit secretaries and nurses should compare patient information on the order form and MAR when transcribing orders. However, ensuring that this information is available to physicians in a way that allows comparison of the identifiers for verification presents a challenge unless computerized prescriber order entry (CPOE) systems are in use.
CPOE systems can be designed so that, once logged on, the physician can select the name from a list of patients assigned to him instead of a much larger list of all patients. In the ambulatory setting, a comparable list would be the schedule of patients who are to be seen that day. Enhancing the font used for the patient’s name on the screen also can improve accurate order entry (for pharmacists, too). Some systems can also alert staff to similar names in the registry and require a second form of identity (e.g., birth date, identification number) before proceeding.
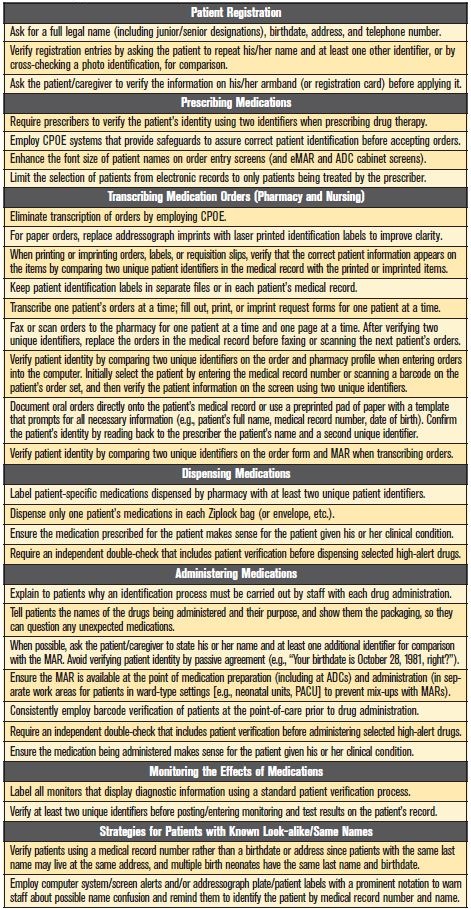
Additional strategies to prevent “wrong patient” medication errors can be found in Table 1.
Reference
- Schulmeister L. Patient misidentification in oncology care. Clinical J Oncol Nurs. 2008;12(3): 495-98.
A short and humorous video about proper patient identification provided by Grey Bruce Health Services in Owen Sound, Ontario, can be viewed here.