
Misidentification of Alphanumeric Symbols in Both Handwritten and Computer-Generated Information
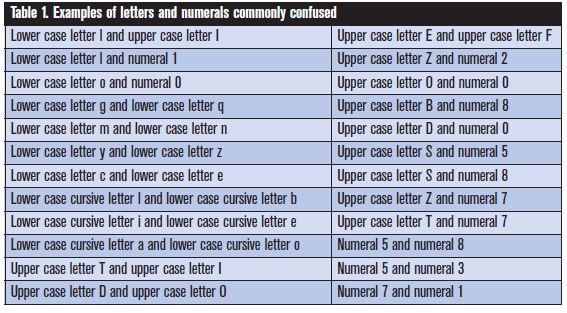
Problem: The English language uses the Latin alphabet with 26 letters and a numeric system with 10 numerals. These alphanumeric symbols (letters and numerals) work well most of the time to communicate information. However, problems may arise during written or electronic communication because of similarities in appearance of the alphanumeric symbols we use. For example, the lower case letter l looks exactly like the numeral 1. The upper case letter O looks like the numeral 0. Since many of the symbols share similar, or even identical, physical characteristics, differentiation often poses a challenge. Table 1 lists examples of commonly confused alphanumeric symbols.
Handwritten information
Mistaken letters and numerals play a large part in errors when reading handwritten drug names and doses. Cursive writing is most susceptible to illegibility and carries the greatest vulnerability to error, as the various symbols often lack distinctiveness.1 A few examples of misinterpreted alphanumeric symbols that happened when reading handwritten medication orders follow.2
Lower case l looks like numeral 1. A nurse misread an order for 2 mg 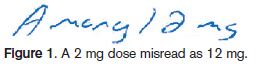 of AMARYL (glimepiride) as 12 mg (see Figure 1).3 The lower case l at the end of the drug name, along with insufficient space between the last letter of the drug name and the dose, led the nurse to misread the dose as 12 mg. The pharmacist processed the order correctly as 2 mg, and the error was detected when the nurse called to question why only 2 mg was dispensed.
of AMARYL (glimepiride) as 12 mg (see Figure 1).3 The lower case l at the end of the drug name, along with insufficient space between the last letter of the drug name and the dose, led the nurse to misread the dose as 12 mg. The pharmacist processed the order correctly as 2 mg, and the error was detected when the nurse called to question why only 2 mg was dispensed.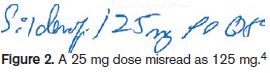 Similar dosing errors have occurred with other drugs with names that end in the letter l (see Figure 2 for another example).4,5
Similar dosing errors have occurred with other drugs with names that end in the letter l (see Figure 2 for another example).4,5
Upper case L looks like upper case I. While reviewing an order for a newly admitted patient, a pharmacist read “IODINE” in the space for allergies. Another pharmacist thought the allergy listed was LODINE (etodolac). The pharmacist contacted the patient’s physician who identified Lodine as the actual allergy.2 The patient was not harmed, but failure to document the correct allergy could have risked serious harm.
Electronic information
Electronic medical records, medication administration records, and computerized prescriber order entry can help overcome many problems with handwritten information. Fortunately, use of such technology is growing. However, even typed or computer-generated physician orders may not prevent confusion among certain alphanumeric symbols. For example, even a clearly typed prescription for 25 mcg of LEVOXYL (levothyroxine) could be misread as 125 mcg if it appears without proper spacing as Levoxyl25 mcg, especially since both strengths are available for this medication.
To cite another example, anyone familiar with email knows how easy it is to misidentify a computer-generated lower case letter l in an email address as the numeral 1, or the letter O as a numeral 0. Information that contains both numerals and letters—including an email address or medication order—is particularly prone to errors. While context can sometimes enhance symbol recognition, it can also detract from recognition. For example, if you saw a Z, I, or O amid an array of numerals, you could easily mistake the symbols as the numbers 2, 1, or 0. Additionally, word recognition software often has difficulty distinguishing L and I, Z and 2, and other look-alike symbols.
Research conducted by Bell Laboratories found that some symbols are more vulnerable than others to misidentification.1 The symbols l and 1, O and 0, Z and 2, and 1 and 7 accounted for more than 50% of the errors caused by symbol misidentification.
Safe Practice Recommendations
There are various ways to help cope with the inadequacies of alphanumeric symbols that are prone to confusion.
Lower case letters or mixed case letters. While there are several handwritten lower case letters that are difficult to distinguish (see Table 1), lower case letters in general offer more differentiation than upper case letters. Mixed case letters (as with tall man lettering) also provide better distinction among letters than using all upper case or all lower case letters.
Block printing on lightly lined forms. Encourage prescribers to use block printing for handwritten orders. Prescribers may save time by using cursive writing, but the time saved needs to be weighed against the risk of error and the tremendous waste of staff time when poorly handwritten orders must be interpreted. Lines on order forms should be lightly shaded, making them visible to prescribers, yet still light enough to prevent interference with symbols—particularly T, 7, and I, or E, F, and L—when reading handwritten and faxed orders.
Symbolic differentiation. Symbolic differentiation is another way to distinctively convey a symbol’s meaning.1 For example, in Europe it’s common to see a zero written with a slash through it (Ø) to differentiate it from the letter O. The numeral 7 can be written with a bar through it to prevent confusion with the numeral 1. The letter Z with a bar through it also can prevent confusion with the numeral 2. Stricter adherence to these principles in the US could help reduce symbol misidentification, although computer software would require changes to allow these slash marks.
Space between the drug name and dose. Allow adequate space between the drug name and the dose on handwritten prescriptions, printed prescriptions and order sets, and electronic formats such as computer selection screens, computer-generated medication labels and records, printed forms, and shelf labels.
Drug and dose make sense. When reading an order, determine if the dose is within a recommended range and available in the strength prescribed. If not, follow-up with the prescriber may be necessary to clarify the order. Keep in mind that the context in which the order is read may not be helpful in all cases to properly identify alphanumeric symbols; however, in the case of medication orders, context may help raise a red flag if the order has been misread.
References:
- Nierenberg GI. Do it right the first time. New York: John Wiley and Sons 1996:154-162.
- ISMP. Misidentification of alphanumeric symbols. ISMP Medication Safety Alert! Acute Care Edition 2000;5(1):1.
- ISMP. Misidentification of alphanumeric characters. ISMP Medication Safety Alert! Community/Ambulatory Care Edition 2003;2(1):3.
- Pennsylvania Patient Safety Authority. What the “l” is the dose? PA PSRS Patient Saf Advis 2006;3(3):19-20.
- ISMP. Tricks but no treats: Illusions and medication errors. ISMP Medication Safety Alert! Acute Care Edition 2002;7(22):1-2.