
Generic Methylergonovine and Engerix-B Mix-Ups Due to Look-Alike Vials
Novartis Pharmaceuticals sent a letter dated July 2012 to hospitals that highlighted the accidental administration of METHERGINE injection (methylergonovine maleate) to newborns instead of hepatitis B injection. Novartis stopped selling Methergine in February 2012 but issued the letter since the company holds the application for the only brand drug product. The letter also mentioned a mix-up between vitamin K and Methergine; however, the mix-up involved oral liquid formulations which are available in Italy. An oral liquid Methergine formulation is not available in the US. Novartis also reported that it had changed the product labeling for Methergine to include information about medication errors, which will be required for the product labeling of generic products in the future.
The brand product Methergine injection used to be packaged in an 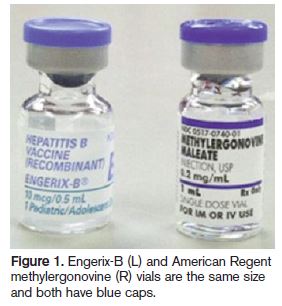 ampul within an amber blister that looked quite different than vials of generic methylergonovine. Now, the generic products are being used exclusively because the brand product Methergine is no longer available. At least two of the recent mix-ups have involved generic methylergonovine distributed by American Regent. Look-alike vials of methylergonovine and ENGERIX-B (hepatitis B vaccine) were mentioned as a contributing factor in both cases (Figure 1).
ampul within an amber blister that looked quite different than vials of generic methylergonovine. Now, the generic products are being used exclusively because the brand product Methergine is no longer available. At least two of the recent mix-ups have involved generic methylergonovine distributed by American Regent. Look-alike vials of methylergonovine and ENGERIX-B (hepatitis B vaccine) were mentioned as a contributing factor in both cases (Figure 1).
In one case, a newborn was accidentally given 1 mL of methylergonovine 0.2 mg/mL instead of Engerix-B. The infant soon developed seizures, rigors, and rigidity that initially went undetected. Both medications were stocked in a profiled automated dispensing cabinet (ADC) refrigerator that was shared between a newborn nursery and the delivery room. The vials were also adjacent to one another.
In the other case, an error happened when a nurse assumed a baby’s care after delivery. The baby had not received the usual newborn medications immediately after birth as ordered, so the nurse felt pressured to administer these medications as soon as possible. Methylergonovine had been brought into the mother’s room along with hepatitis B injection and other medications for the baby, who was also in the mother’s room. The hepatitis B vaccine was accidentally knocked under a towel, and the nurse did not notice that she was actually holding a vial of methylergonovine, not hepatitis B vaccine. She noticed the blue cap, which she knew was on an Engerix-B vial, but did not recognize that the blue cap was actually on the American Regent methylergonovine vial. The hospital used a point-of-care bedside barcoding system, but the newborn’s identification (ID) bracelet had not been prepared yet. Due to perceived time pressures, the baby was given the medication instead of waiting for the barcoded ID bracelet so the baby and drug could be scanned. When the baby’s ID bracelet arrived, the nurse scanned the medications and discovered the error. The baby was monitored and recovered without sequelae.
Norvartis made several recommendations in its letter, which we endorse. The company suggested separating newborn medications from those typically used for mothers in perinatal areas of the hospital. If an ADC must be shared between these units, a locked, lidded storage bin should be used for pediatric products and the selection screen should highlight which medications are for the mother and which medications are for the infant. If possible, infant medications should be administered in an area that is separate from where medications are administered to the mother. This strategy may not be workable in hospitals where mothers and babies room together. However, many infants are initially evaluated in a newborn nursery setting, so administration of some medications after birth, including hepatitis B vaccine, may be delayed until the baby is in the nursery. Finally, hospitals should implement workflow processes in which infants can be reliably banded with an ID bracelet immediately after birth. Delaying the application of ID bracelets on newborn infants simply invites barcode technology workarounds.