
Fluorouracil Error Ends Tragically, But Application of Lessons Learned Will Save Lives
In August 2006, a 43-year-old Canadian woman with advanced nasopharyngeal carcinoma died as a result of an accidental overdose of fluorouracil. ISMP Canada, our North American sister organization, was invited to perform a root cause analysis (RCA) of the event.1,2 As mentioned in our May 17, 2007 newsletter, the provincial cancer board where the event happened took an exceptional step and made the RCA report available on the Internet to promote learning across the country. In cooperation with ISMP Canada, we offer a summary of the error, examples of causative factors, and highlights of recommendations to address the causative factors, as the lessons learned from this tragedy are applicable to any organization that provides oncology services.
Summary of the Event
In July 2006, the patient was being treated in an ambulatory clinic according to a protocol that included high-dose fluorouracil and cisplatin. On the day of the event, the patient received 5,250 mg of fluorouracil (4,000 mg/m2) over 4 hours instead of 4 days, as intended. The order for fluorouracil was written as follows:
5-Fluorouracil 5250 mg (at 4,000 mg/m2) intravenous once continuous over 4 days... Continuous infusion via ambulatory infusion pump (Baseline regimen dose = 1000 mg/m2/day = 4000 mg/m2/4 days).
After the nurse reviewed the patient’s orders, lab results, height, and weight, a pharmacy technician prepared the medications (fluorouracil and cisplatin) and a pharmacist checked them before dispensing them to the clinic. The fluorouracil bag contained about 130 mL of solution (final concentration of 45.57 mg of fluorouracil/mL) before priming the IV administration set. The nurse used a calculator to determine the infusion rate and programmed the infusion pump (Abbott AIM Plus—no longer marketed in the US) to deliver the fluorouracil at 28.8 mL/hour. However, 28.8 mL was the total volume of solution that should have been infused in 24 hours, not 1 hour. The correct hourly infusion rate was 1.2 mL. Another nurse was asked to confirm the calculation. She could not find a calculator, so she did the math in her head and on a scrap of paper but did not pick up the miscalculation by the first nurse. The infusion was started and the patient was discharged with instructions to return for pump discontinuation 4 days later. The patient also received 100 mg of IV cisplatin that day.
Four hours after discharge, the patient noticed that the pump was beeping and that the IV bag was empty. The patient returned to the clinic immediately, where the error was recognized. An evening nursing supervisor notified an on-call physician about the mistake, who suggested there was no treatment and that the patient should call again the next morning. The error was disclosed to the patient, and she was advised to stay hydrated. A unit manager called the patient the next morning, advised her of possible serious side effects, and asked her to come to the facility for monitoring. The patient was feeling well and preferred not to come to the facility. When the patient’s attending physician became aware of the mistake, he conducted a literature search for potential treatment options. The patient was notified and advised to call if she developed any sign of mouth sores. Two days after the event, the physician called to check on the patient and arrangements were made for her to come in the following day for assessment, although she was still feeling well. When seen in the clinic the next day, the patient was complaining of nausea, vomiting, and throat discomfort. She was treated and discharged, and admission to the hospital was arranged for the next day, as no beds were then available. The following day, the patient was hospitalized. During the following weeks, she developed profound mucositis and pancytopenia, hemodynamic collapse, and multi-organ failure. Sadly, the patient died 22 days after the event. Unfortunately, the design of the treatment protocol (4 days of high-dose fluorouracil in one infusion bag, combined with a single 100 mg dose of cisplatin) increased the likelihood that this would happen. The cause of death was determined to be sequelae of fluorouracil toxicity, cumulative with cisplatin toxicity. ISMP Canada found that other fatal errors with fluorouracil had occurred in North America at least seven times in the past.
Examples of Causative Factors
Miscalculation. The nurses who programmed the pump and verified the settings carried out complex 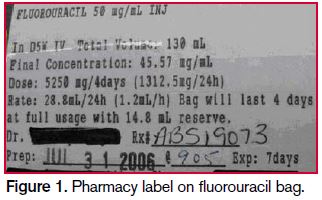 calculations at the bedside to determine the infusion rate (mL/hour). Both omitted a step in the calculations, forgetting to divide the daily dose by 24 hours. As seen in Figure 1, the mL/hour infusion rate did appear on the label of the infusion bag, although not prominently. The nurse did not notice that the infusion would last only 4 hours at her calculated rate of infusion.
calculations at the bedside to determine the infusion rate (mL/hour). Both omitted a step in the calculations, forgetting to divide the daily dose by 24 hours. As seen in Figure 1, the mL/hour infusion rate did appear on the label of the infusion bag, although not prominently. The nurse did not notice that the infusion would last only 4 hours at her calculated rate of infusion.
Design of pharmacy label. The pharmacy label was difficult to read and unnecessarily listed the mL/24 hours rate of infusion (28.8 mL/24h) first, and then the mL/hour infusion (1.2 mL/h) in parentheses (see Figure 1). The nurses who miscalculated the hourly rate exhibited confirmation bias, as they thought their erroneous calculations were correct when they saw ‘28.8’ as the first entry for ‘rate’ on the label. The nurses did not realize that the pharmacy had listed the mL/24 hours rate of infusion on the label before the mL/hour rate of infusion.
Failed double-check system. The nurse who was asked to double-check the initial infusion rate calculation was distracted and on the way to perform another task at the time. She could not find a calculator, so she performed the calculation mentally and on a scrap of paper. The checking process was informal and unstructured, and there was no requirement to perform calculations independently or to document calculations or any other aspects of a checking process.
Complex workload. The work processes on the unit required multitasking, and the various tasks that needed to be accomplished (e.g., checking lab results; weighing the patient; assessing the patient’s condition; reviewing the order, label, and calculations; programming the pump; educating the patient) were not sequenced in a stepwise fashion. Many high-risk tasks, including attending to the infusion pump, were performed simultaneously with other tasks.
Pump design contributions. Human factors design flaws with the pump increased the cognitive load associated with programming the pump. For example, programming choices were listed as mg/mL, µ/mL, or mL (meaning mL/hour); the prompt for container size actually required entry of the volume to be infused; and the review screen did not provide data about the duration of the infusion that had been programmed. Also, the pump was not a smart pump, so it lacked dosage error-reduction software that could detect excessive doses or programming errors.
Lack of familiarity with protocol. The nurse who programmed the pump had a low index of suspicion regarding the high infusion rate. She was new to the unit and had never administered a 4-day fluorouracil infusion. The calculated rate of 28.8 mL/hour was not unusual compared to other infusions delivered in the clinic.
Unprepared to manage overdoses. Staff were uncertain how to best treat and support the patient after the overdose was detected. Depending on the degree of toxicity that occurs with chemotherapy, patients who receive prompt treatment of overdoses or serious adverse effects from prescribed doses of chemotherapy may be less likely to experience irreversible harm.
Safe Practice Recommendations
Standardize how key information is displayed on pharmacy labels. Ensure that the information needed to program an infusion pump (e.g., total volume, concentration, hourly rate of infusion) is prominently displayed in a standard and consistent way on pharmacy labels. Eliminate extraneous information, such as mL/24 hours, as infusion rates should be communicated as an hourly rate. Consider human factors design principles to improve readability. Ensure that pharmacy staff are familiar with the pumps in use and the programming processes.
Review chemotherapy certification processes. Review the processes by which certification is granted to nurses who administer chemotherapy, and make any changes necessary to ensure that staff exhibit and maintain an appropriate level of skills, knowledge, and abilities before working independently.
Use pumps with safeguards. To our knowledge, smart pumps for use in ambulatory care settings are not currently available. When they do become available, their use should be encouraged to maximize safety features such as dose alerts, dosing and flow rate limits, and operator feedback to allow detection of pump programming errors. Conduct usability testing and a failure mode and effects analysis to evaluate pumps in current use and under consideration for purchase, to uncover risks and reduce the chance of programming errors. Use one type of ambulatory pump throughout the organization.
Enhance independent double-checks. Develop a structured process for conducting and documenting independent double-checks, and incorporate instruction related to this process into staff orientation and annual competencies. (See our May 31, 2007, newsletter for details about effective, independent double-check processes.) Promote critical thinking during the preparation and checking of all chemotherapy. Design checklists to facilitate compliance with all the steps necessary for safe dispensing and administration of chemotherapy, including a specific checklist to guide the verification process and to promote documentation of the check process. Minimize the need for calculations as much as possible.
Review pump screens with patient. Include a review of pump data-input screens when teaching patients about their therapy, in order to provide a final opportunity for practitioners to review data input and possibly detect incorrect programming.
Define treatment protocols for accidental overdoses. Define a treatment protocol for fluorouracil overdose and include the provision of aggressive supportive care in the immediate treatment plans for such overdoses (e.g., hospitalization, IV hydration and forced diuresis, timely administration of hematopoietic growth factors, prophylactic antibiotics). Require all staff who prescribe, dispense, and administer chemotherapy to demonstrate proficiency in identifying and managing chemotherapy-induced toxicities.
For complete details of the RCA, readers are encouraged to review the full report, listed below in Reference 1.
References:
- ISMP Canada. Fluorouracil incident root cause analysis. April 30, 2007
- ISMP Canada. Fluorouracil incident RCA: follow-up. ISMP Canada Safety Bulletin 2007;7(4): 1-4.