
Dakin's Solution Accidentally Given IV
Problem: A woman was admitted to a hospital with serious burns on her left arm. Dakin’s solution (diluted sodium hypochlorite solution) was ordered for topical wound irrigation. At the same time, an IV was also started in the patient’s left arm, near the wound, but was later capped when a peripherally inserted central catheter (PICC) was placed in the right arm. The IV access in the left arm was not removed because it was partially covered by the burn dressing. The day nurse did not communicate with the night nurse to tell her that the IV in the left arm should be removed at the next dressing change. Also, the ordering physician changed the wound care to silver sulfadiazine cream but forgot to discontinue the Dakin’s solution. So the patient’s night nurse believed the irrigations with Dakin’s solution were to be continued.
The solution was in a commercially available bottle in the patient’s room. It was poured into a sterile bowl from which it was drawn into a syringe so it could be used to irrigate the wound. Lines for wound irrigation were normally labeled. Although the capped IV catheter in the patients left arm was not incorrectly labeled as an irrigation catheter, the nurse assumed it was an irrigation catheter under the dressing and, therefore, administered Dakin’s solution via the capped IV catheter. Fortunately, the patient called out when the solution began burning as it was being administered. The nurse immediately removed the dressing, realized the Dakin’s solution was being given IV, and stopped administration after only 15 mL or less had been given. The patient recovered without sequelae.
Safe Practice Recommendations
Tracing tubing and catheters to the point of origin is currently the primary way to prevent catheter misconnections, although in this case, the access site was covered with a dressing. The facility where this event happened is reevaluating catheter placement near wound dressings and considering how to differentiate IV catheters from wound catheters. Clearly visible labels on access lines that are covered with dressings or clothing might help prevent misconnections.
Another facility where a similar misconnection occurred is now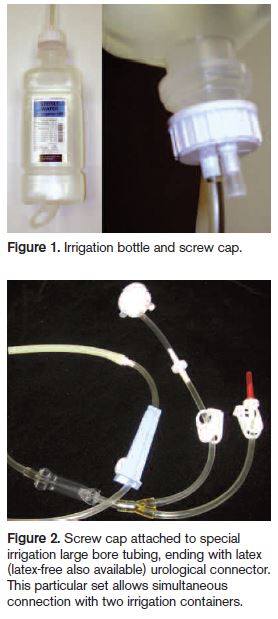 using a special set-up for burn irrigations. They use a sterile water for irrigation container from Hospira along with a 38 mm screw cap. The long plastic tube coming from the cap is coupled with the spike of an irrigation administration set, also from Hospira (see Figure 1). This is available with special, large bore tubing and a urological connector that won’t connect to an IV catheter (see Figure 2). A similar set-up may be available from other vendors. Check with your salesperson for the correct catalog number as various set-ups exist. Even if a similar system isn’t used, we’d highly recommend that irrigations always be prepared in the pharmacy and placed in containers that are dissimilar to IV containers, such as the Hospira container mentioned above. Although that wouldn’t have helped here, since the catheter was confused, it’s still an important consideration to prevent container mix-ups.
using a special set-up for burn irrigations. They use a sterile water for irrigation container from Hospira along with a 38 mm screw cap. The long plastic tube coming from the cap is coupled with the spike of an irrigation administration set, also from Hospira (see Figure 1). This is available with special, large bore tubing and a urological connector that won’t connect to an IV catheter (see Figure 2). A similar set-up may be available from other vendors. Check with your salesperson for the correct catalog number as various set-ups exist. Even if a similar system isn’t used, we’d highly recommend that irrigations always be prepared in the pharmacy and placed in containers that are dissimilar to IV containers, such as the Hospira container mentioned above. Although that wouldn’t have helped here, since the catheter was confused, it’s still an important consideration to prevent container mix-ups.
In 2005, we wrote about a similar catheter misconnection problem with the V.A.C. INSTILL SYSTEM by KCI. This is a wound healing system that facilitates automated delivery of topical solutions to wound sites. Unfortunately, the device is designed to accommodate IV tubing to deliver the topical solution. Please refer to the article linked below if you are using or contemplating use of this device, as additional prevention measures will apply (www.ismp.org/newsletters/acutecare/articles/20051006-1.asp).