
Any New Process Poses a Risk for Errors: Learning from 4 Months of Coronavirus Disease 2019 (COVID-19) Vaccinations
Problem: The Pfizer-BioNTech and Moderna mRNA coronavirus disease 2019 (COVID-19) vaccines were granted emergency use authorization (EUA) by the US Food and Drug Administration (FDA) in mid-December 2020. Between December 14, 2020 (the date COVID-19 vaccinations began) and April 17, 2021, more than 107 million doses of the Pfizer-BioNTech vaccine and nearly 91 million doses of the Moderna vaccine had been administered in the US.1 At the end of February, FDA granted EUA to a third COVID-19 vaccine, a human adenovirus viral vector vaccine from Janssen (Johnson & Johnson). As of April 13, 2021, nearly 8 million doses of the Janssen vaccine had been administered in the US.1 Out of an abundance of caution, the Centers for Disease Control and Prevention (CDC) and FDA recommended pausing use of the Janssen vaccine on April 13, 2021, due to reports of a rare and severe type of blood clot (cerebral venous sinus thrombosis [CVST] with thrombocytopenia) in six women between the ages of 18 and 48, which occurred 6 to 13 days after receiving the Janssen vaccine.2,3 CDC and FDA continue to investigate the potential role of the vaccine in this adverse event, especially since similar rare adverse events have been reported with the AstraZeneca COVID-19 vaccine, also an adenovirus (chimpanzee) viral vector vaccine, administered in Europe.4
In our January 14, 2021 newsletter, we published an analysis of the early vaccine errors we had received in the first month of administering the Pfizer-BioNTech and Moderna vaccines.5 Now that the US has been administering COVID-19 vaccines for about 4 months, we have analyzed more than 160 COVID-19 vaccine errors voluntarily reported to ISMP between December 14, 2020, and April 15, 2021. The errors reported to ISMP do not reflect all COVID-19 vaccine errors that might be occurring nationally; in fact, the CDC has received more than 300 inquiries from practitioners seeking guidance for managing COVID-19 vaccine administration errors.6,7 Because COVID-19 vaccine errors could result in reduced effectiveness, adverse drug events, and other safety implications, we want to share what we have learned about these errors and recommend best practices.
In our January analysis, most reports were associated with dilution errors (Pfizer-BioNTech vaccine), wasted vaccine doses, administration to the wrong age group, and errors associated with scheduling second doses.5 While these error types continue to be reported, we are now receiving a wide variety of different error report types. During our analysis, each COVID-19 vaccine error report was categorized into one of four broad categories: general error types, errors specific to the two-dose vaccines, dilution errors with the Pfizer-BioNTech vaccine, and errors specific to the single-dose vaccine (Table 1). The following includes a description of each error type along with an example of a reported error. We conclude with safe practice recommendations to help prevent these types of errors. Please note: While ISMP has NOT received any reports of CVST or other adverse reactions to the Janssen vaccine, recommendations based on our analysis include best practices associated with a single-dose vaccine like the Janssen vaccine, despite its current pause in administration (which is expected to end soon).
Table 1. Types and percentages of COVID-19 vaccine errors reported to ISMP (December 14, 2020, to April 15, 2021)
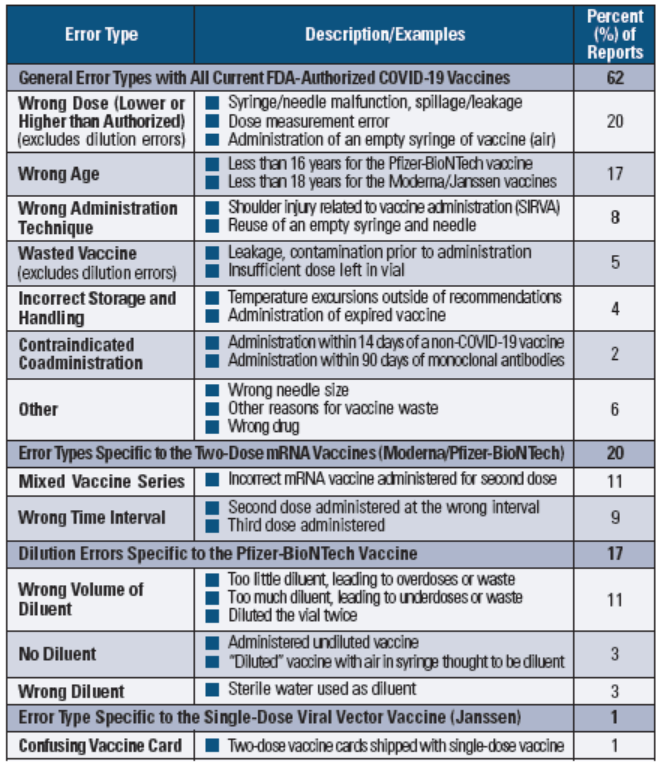
General Error Types with All Current FDA-Authorized COVID-19 Vaccines
Reports grouped into this general category predominately included error types associated with any of the FDA-authorized COVID-19 vaccines:
-
Administration of a dose lower than authorized, often due to the patient pulling away during vaccination, leftover vaccine in the syringe after injection, or vaccine leakage during injection (e.g., premature retraction of a VanishPoint syringe needle, leakage with a Guangdong Haiou Medical Apparatus Company syringe—see a related Safety Brief in the right column)
At a mass vaccination clinic, about 4,300 patients received 0.2 mL instead of 0.3 mL doses of the Pfizer-BioNTech vaccine. The orange-capped syringes from a national stockpile left about a third of the vaccine stuck in the bottom of the plastic syringe.8
-
Administration to a patient younger than authorized (less than 16 years for the Pfizer-BioNTech vaccine, less than 18 years for the Moderna and Janssen vaccines), often because the vaccine provider did not ask age-related screening questions
Office staff were covering for a vaccine coordinator when a 16-year-old teen arrived with her mother, who wanted the teen immunized so she could visit a sick relative. The teen received the Moderna vaccine despite her unauthorized age.
-
Administration using the wrong injection technique, which often resulted in a shoulder injury related to vaccine administration (SIRVA)
A first responder received a vaccine too high in the shoulder from a volunteer nurse, leading to physician confirmation of SIRVA requiring possible surgical repair. The first responder’s supervisor did not report the event to FDA. Five weeks later, the first responder is still in pain and has limited mobility of the arm or shoulder.
Additional reports in this category included:
-
Administration of a dose higher than authorized (e.g., 1 mL instead of 0.5 mL dose for the Moderna vaccine)
-
Using the wrong needle size (e.g., needle length 5/8 inch instead of 1 or 1.5 inches)
-
Administration of an empty vaccine syringe (e.g., previously used syringe, sterile syringe with the plunger pulled back in preparation for vaccine or diluent withdrawal and air mistaken as vaccine)
-
Incorrect vaccine storage and handling, leading to vaccine waste or administration of expired vaccine
-
Other reasons for vaccine waste (e.g., inadvertent disposal, vaccine spillage)
-
Administration of the wrong drug (e.g., EPINEPHrine in a pharmacy-prepared syringe instead of a vaccine in a pharmacy-prepared syringe)
-
Coadministration within 14 days of a non-COVID-19 vaccine and within 90 days of a monoclonal antibody used as part of a COVID-19 treatment
Error Types Specific to the Two-Dose mRNA Vaccines (Moderna/Pfizer-BioNTech)
Two error types were reported that were specific to the two-dose mRNA vaccines:
-
Administering the wrong mRNA vaccine for the second dose, often due to scheduling patients to receive their second dose on days the site only administered one type of mRNA vaccine (which did not match the patient’s first dose), or not verifying the manufacturer documented on the patient’s vaccine card (or medical record or state/local immunization information system [IIS]) at the time of vaccination
A patient received the Pfizer-BioNTech vaccine for the second dose instead of the Moderna vaccine. The vaccination site administered the different vaccines in two separate rooms. The patient joined the wrong line after checking in. The patient’s vaccine card had been checked during the screening process but did not accompany the patient into the vaccination room. Prior to vaccination, the nurse did not believe she needed to verify the manufacturer since the patient had already been screened.
-
Wrong interval errors in which a second vaccine dose was administered too soon outside of the CDC-allowable 4-day grace period (less than 17 days [Pfizer-BioNTech] or 24 days [Moderna] after the first dose) or too late (more than 42 days after the first dose), or a third dose was inadvertently administered
A second dose of the Moderna vaccine was administered 2 weeks early. The patient completed a questionnaire stating that she had not received a first dose of the vaccine. During a verbal interview, the patient did not say she had received the first Moderna vaccine dose 2 weeks earlier at a different facility and did not produce a vaccine card. The error was noticed when documenting vaccine administration in the state IIS. When the patient was called about the error, she said she had just answered “No” to all the questions without reading them.
Dilution Errors Specific to the Pfizer-BioNTech Vaccine
Dilution errors related to the Pfizer-BioNTech vaccine were grouped into the following error-type categories:
-
Using the wrong volume of diluent, including too little diluent, too much diluent, or diluting the vaccine vial twice
A nurse diluted the same vaccine vial twice using 1.8 mL of 0.9% sodium chloride each time. She was distracted after the initial dilution. When she returned to the task, she picked up the same vial and diluted it again. She noticed the extra volume in the vial before administration. The vial of vaccine was discarded.
-
Using the wrong diluent, mostly sterile water instead of 0.9% sodium chloride
The Pfizer-BioNTech vaccine had been delivered to a hospital pharmacy, but the diluent remained in the truck that delivered the vaccine. A technician diluted the vaccine with sterile water, and the pharmacist who checked the diluent before it was added did not notice the error given the similarity of sterile water and 0.9% sodium chloride vials. Two doses were administered before the pharmacist noticed the error.
-
Not diluting the vaccine, leading to administration of undiluted vaccine
A nurse thought she had injected 1.8 mL of diluent into the vaccine vial. She withdrew the first dose of 0.3 mL and administered it, but the second dose was an insufficient volume. The nurse determined that air had been injected into the vaccine vial rather than the diluent.
Error Type Specific to the Single-Dose Viral Vector Vaccine (Janssen)
While we received numerous error reports associated with the Janssen vaccine that fall within the general category listed above, only one report was specifically related to a single-dose COVID-19 vaccine. As noted in a previous newsletter, current Vaccination Record Cards provided by the government include spaces to document two doses of the Moderna and Pfizer-BioNTech vaccines, along with a reminder to schedule the second dose.9 This could cause confusion for patients receiving the single-dose Janssen vaccine. An update to the Vaccination Record Card for the single-dose vaccine is not being considered.
Safe Practice Recommendations: Millions of doses of the COVID-19 vaccines will be administered over the next few months. As we work toward expanding vaccinations to all, we must also learn from the vaccine errors that have already happened and implement strategies to minimize the risk of making these same vaccine errors. Consider the following targeted recommendations:
Staff competency
-
Educate and orient all vaccination staff (including volunteers) regarding their role in COVID-19 vaccination check-ins, patient screening, preparation, and/or administration, as well as the common error types that may occur.
-
Verify the competency of all vaccinators, particularly regarding:
-
Age indications for each vaccine
-
Proper dilution of only the Pfizer-BioNTech vaccine
-
Proper dose withdrawal technique
-
Timing and scheduling of a second vaccine dose (if needed)
-
-
Verify the competency of all staff who check-in and screen patients for vaccination, particularly regarding:
-
Age indications for each vaccine
-
Timing and scheduling of a second vaccine dose (if needed)
-
Screening patients for allergies, prior vaccinations, prior administration of monoclonal antibodies used to treat COVID-19, and other health indicators
-
Verifying the first vaccine (date, manufacturer) via the state/local IIS, medical record, and/or the patient’s vaccine card for patients requiring a second dose
-
Patient scheduling and check-in process
-
Schedule patients for a second dose (if needed) before they leave the vaccination site after receiving their first dose.
-
Establish a vaccination scheduling system that does not allow patients younger than 16 years to obtain an appointment, and schedules appointments for patients who are 16 and 17 years old only for administration of the Pfizer-BioNTech vaccine.
-
During the check-in process:
-
Ask patients age-related screening questions including their date of birth. Strictly comply with vaccine age restrictions.
-
Check the state/local IIS for documentation of a previous COVID-19 vaccine for all patients requesting a first or second vaccine dose. Require all patients who arrive for a second dose to present their vaccine card and have them carry the card throughout the process so the vaccinator can verify the information.
-
Preparation process
-
If feasible within the timeframe for vaccine stability at room temperature, have the pharmacy verify the number of vaccines needed each day (to prevent waste) and dispense prefilled, labeled syringes of the vaccine to vaccination clinics.
-
In the pharmacy:
-
Stock vials of sterile water in a different location than 0.9% sodium chloride
-
Separate the preparation of each brand of vaccine
-
Withdraw doses from one vaccine vial at a time before accessing the next vial
-
Label vaccine syringes immediately after preparation
-
-
Remove syringes from their packaging one at a time immediately before drawing up diluents or doses; do not open syringe packages ahead of time and/or fill syringes with air in preparation for later dose or diluent withdrawal.
Administration process
-
Stock each vaccination station with a sharps container for syringe/needle disposal.
-
Before administration of any dose, check the syringe for the correct dose volume, air bubbles, and a tight fit between the needle hub and the syringe.
-
Before administration of a second dose, visually check the patient’s vaccine card to verify the correct time interval and manufacturer.
-
If preparing the Pfizer-BioNTech vaccine outside of the pharmacy, require an independent double check of the dilution process (if staffing permits).
-
After administration, immediately engage the needle safety device and dispose of the syringe in a sharps container (do not leave the used syringe on the table).
-
Report any syringe or needle malfunctions to the pharmacy.
-
After administration, complete the patient’s vaccine card. For single-dose COVID-19 vaccines, cover all references to a second dose (front and back of the card) with a note that only a single dose is required.
-
Stock the vaccination site with EPINEPHrine autoinjectors rather than prefilled syringes to visually differentiate EPINEPHrine injections from vaccine syringes.
If an error happens
-
Always inform the patient of a vaccine administration error.
-
Click here for a table published by the CDC that provides interim recommendations for actions to take after an error has happened.7
-
Determine how the error occurred and implement strategies to prevent it from happening again.
-
Providers are required to report all COVID-19 vaccine administration errors—even those not associated with an adverse event—to the Vaccine Adverse Event Reporting System (VAERS). Also report significant adverse events (including SIRVA) following vaccination, cases of multisystem inflammatory syndrome, and cases of COVID-19 in immunized patients that result in hospitalization or death, even if you are not certain that the vaccination was related to the event.
-
Also report COVID-19 vaccination errors to ISMP to promote shared learning opportunities.
References
- Haseman J. Tracking COVID-19 vaccine distribution by state: how many people have been vaccinated in the US? USA Today. January 14, 2021. Updated April 18, 2021.
- Centers for Disease Control and Prevention (CDC). Recommendation to pause use of Johnson & Johnson’s Janssen COVID-19 vaccine. Updated April 20, 2021.
- Oliver S, Shimabukuro T. Johnson & Johnson/Janssen COVID-19 vaccine and cerebral venous sinus thrombosis with thrombocytopenia – update for clinicians on early detection and treatment. Clinical Outreach and Communication Activity (COCA) webinar. April 15, 2021.
- European Medicines Agency (EMA). AstraZeneca’s COVID-19 vaccine: EMA finds possible link to very rare cases of unusual blood clots with low blood platelets. Published April 7, 2021.
- Institute for Safe Medication Practices (ISMP). Learning from errors with the new COVID-19 vaccines. ISMP Medication Safety Alert! Acute Care. 2021;26(1):1-5.
- Schillie SF, Buzzell J, Nelson CA, Kidd S, Shealy KR, Reagan-Steiner S. Common COVID vaccine administration errors to watch for. Medscape. April 9, 2021.
- Centers for Disease Control and Prevention (CDC). COVID-19 vaccine: administration errors and deviations. Published March 17, 2021.
- Fernandez L. Thousands at Oakland Coliseum received wrong vaccine dosage, medical staff say. KTVU Fox 2. March 3, 2021.
- Institute for Safe Medication Practices (ISMP). Vaccine card incorrect for single-dose COVID-19 vaccine. ISMP Medication Safety Alert! Acute Care. 2021;26(6):1-2.
Access this Free Resource
You must be logged in to view and download this document.