
Administering a Saline Flush “Site Unseen” Can Lead to a Wrong Route Error
Problem: Earlier this year, ISMP learned about an event that resulted in the administration of a saline flush solution by the wrong route. In an unusual twist, the saline flush was administered by a laboratory technician who was attempting to collect blood samples from what she thought was a central venous access device (CVAD). The saline flush was instead administered via extension tubing that was connected to a continuous peripheral nerve block infusion.
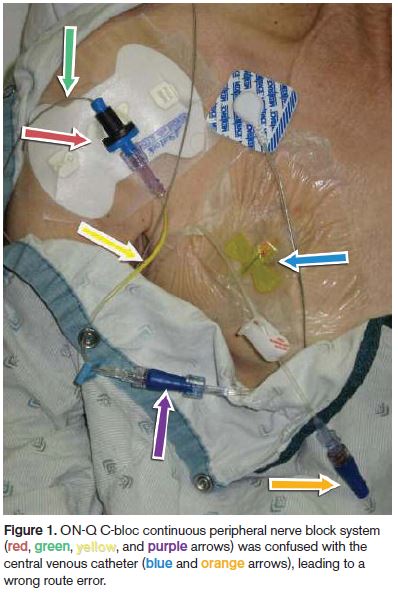 Prior to the event, an anesthesia practitioner had placed an ON-Q C-bloc continuous peripheral nerve block system in the patient’s thoracic paravertebral region to help control pain. The ON-Q system catheter (green arrow, Figure 1) that bathed the thoracic region with a local anesthetic was anchored at the patient’s right shoulder using a large white stabilization device (red arrow). Typically, anesthesia staff place the stabilization device on the back of a patient’s shoulder. In this case, placing the stabilization device on the front of the shoulder, presumably to promote comfort, contributed to mistaking the ON-Q system tubing as the CVAD catheter, which was also located near the patient’s right shoulder (blue arrow).
Prior to the event, an anesthesia practitioner had placed an ON-Q C-bloc continuous peripheral nerve block system in the patient’s thoracic paravertebral region to help control pain. The ON-Q system catheter (green arrow, Figure 1) that bathed the thoracic region with a local anesthetic was anchored at the patient’s right shoulder using a large white stabilization device (red arrow). Typically, anesthesia staff place the stabilization device on the back of a patient’s shoulder. In this case, placing the stabilization device on the front of the shoulder, presumably to promote comfort, contributed to mistaking the ON-Q system tubing as the CVAD catheter, which was also located near the patient’s right shoulder (blue arrow).
When placing the ON-Q system in the patient’s paravertebral region, anesthesia staff decided to attach a short extension set with yellow-striped tubing (yellow arrow) to warn staff that the infusion was not being administered intravenously but rather into the paravertebral region. Before this instance, yellow-striped tubing had been reserved for epidural infusions only. Because the extension set had been added, a MicroClave connector (purple arrow) had to be used to connect the yellow-striped tubing to the main tubing of the ON-Q system. This type of connector is commonly used with CVADs (orange arrow).
When the technician went to withdraw blood from the patient, the upper part of the patient’s gown obscured the ON-Q C-bloc system affixed to the upper right shoulder; only the CVAD insertion site was visible (blue arrow). The yellow-striped tubing and the connector (purple arrow) associated with the ON-Q system were also visible, giving the appearance that they were actually attached to the CVAD. The technician was familiar with the connector because these were frequently used with CVADs. The technician had difficulty disconnecting the connector from the tubing so she could withdraw the blood specimens. She left the patient’s room and asked a busy nurse for help. The nurse did not remember that the patient’s CVAD was capped and did not need to be disconnected from an infusion. She gave the technician a hemostat, which helped remove the tubing from the connector. The technician attempted to confirm placement of the CVAD but could not obtain a blood return. She then flushed the line with normal saline, which infused into the paravertebral region. Fortunately, the patient was not injured. The inability to collect the blood specimens led the technician to seek additional help from the nursing staff, which then led to the discovery of the error.
Safe Practice Recommendations: According to the Association for the Advancement of Medical Instrumentation (AAMI), a year from now, hospitals will likely start to see newly designed connectors on medical tubing on the market—the end result of a joint working group that is developing standards that will make misconnections virtually impossible because the design of the connectors will no longer be universal as it is now with Luer connectors. Instead, the design of each connector will be specific to its application. The first Provisional American National Standards to be released in 2014 are associated with connectors for enteral applications, limb inflation applications (e.g., blood pressure cuffs, limb compression devices), and Luer connectors, which will then be followed by neuraxial applications later in 2014. But there isn’t anything on the horizon that would prevent a Luer connector on a syringe used to withdraw blood from being connected to tubing used for the delivery of regional anesthetics via the ON-Q systems. Considering all the elements that contributed to this particular event, please take the following precautions to prevent a similar error in your organization.
Limit access. Limit access to CVAD lines for any purpose, including blood collection, to those with professional healthcare training and demonstrated competencies; these staff are more likely to know and follow safety measures associated with these devices and are more likely to be knowledgeable about the serious ramifications of misconnections, infections, occlusions, or misadministration of medications. For example, given the risk of occlusion and infection alone, most hospitals do not allow laboratory technicians to draw blood from CVADs. Some hospitals prohibit technician access to these catheters in certain settings, such as critical care units, or for certain patient groups, such as bone marrow transplant patients (as did the hospital where the error occurred). However, international guidelines from the World Health Organization (WHO) suggest that the best practice is to only allow trained nursing staff and physicians to access central venous lines for blood specimen collection.
Trace access lines. Promote a consistent process for tracing all catheters/lines from the access site into the patient’s body all the way to the end source of an infusion or capped access port before drawing blood, connecting or reconnecting tubing, and/or administering drugs, solutions, flushes, or other products. Remind staff that, for patients with multiple tubes and catheters, situational awareness of each tube’s location and insertion site can be lost, especially if tubing is obscured by clothes and bed sheets. It is also important to fully uncover the insertion site before access is attempted, otherwise mix-ups between look-alike tubing and devices can lead to serious wrong route errors.
Communicate practice changes. Changes in dressing locations, types of tubing and connectors, and other altered practices should be readily communicated with all members of the healthcare team who are providing care to the patient.
Provide training. Educate all staff who might use or encounter ON-Q C-bloc, ON-Q PainBuster, or other new tubes, catheters, connectors, or drug delivery systems regarding proper use or access. Include discussions about possible sources of errors and steps to avoid these errors (see our July 16, 2009 issue for more strategies to prevent errors with ON-Q pumps). When possible, include tubing misconnections in simulation training during orientation and annual safety competencies.
Label lines. Affix labels on lines if the patient has more than one potential connection to a port of entry into the body (e.g., IV, arterial, umbilical, enteral, bladder, drainage tubes). For the ON-Q C-bloc infusions, affix labels indicating “CONTINUOUS NERVE BLOCK” to alert staff, particularly given that, in many hospitals, only anesthesia staff can manipulate these catheters or dressings.
Use epidural tubing appropriately. Avoid use of yellow-striped tubing for anything other than its intended purpose: administration of epidural infusions; its use in other circumstances could result in unintended negative consequences, as it did in this case. When possible, avoid use of any extension sets with the ON-Q C-bloc infusions or tubing connectors that may resemble those used with CVAD catheters and tubing.
Additional strategies. For addressing the wide-ranging potential for tubing misconnections, hospitals might also want to conduct a self assessment to identify all products and practices that pose a risk of inadvertent tubing misconnections, with the goal of mitigating identified risks. A tool created in 2012 by Baxter in cooperation with ISMP guides users through a modified risk assessment that evaluates current delivery systems and mating devices, rating ease of connection and potential for patient harm, and assigning a risk priority score. The full assessment and tutorial can be accessed from Baxter’s Clinical Center of Excellence website.