
Your High-Alert Medication List—Relatively Useless Without Associated Risk-Reduction Strategies
Problem: Have you ever watched the 1993 movie, Groundhog Day? Bill Murray plays Phil Conners, a television news reporter who finds himself reliving the same day over and over again—a much-hated assignment covering the annual Groundhog Day event in Punxsutawney, PA. Well, at times it feels like “Groundhog Day” when we hear about the same types of errors happening over and over again. Another patient with diabetes receives a 5-fold overdose of U-500 insulin after a nurse draws the dose into a U-100 syringe, and a double-check by another nurse fails to detect the error. Another hospitalized patient experiencing pain receives an overdose of intravenous (IV) HYDROmorphone after a physician prescribes the IV dose in the same amount as the oral dose the patient had been taking at home, and neither the pharmacist nor nurse captures the error. Another woman receives a rapid infusion of magnesium sulfate postpartum instead of oxytocin, despite staff awareness of prior mix-ups.
In many cases, events like these and others continue to happen in hospitals with medications that are on the hospital’s list of high-alert medications. High-alert medications are drugs that bear a heightened risk of causing significant patient harm when they are used in error. Although mistakes may or may not be more common with these drugs, the consequences of an error with these medications are clearly more devastating to patients. This is repeatedly borne out in the literature1-5 and by reports submitted to the ISMP National Medication Errors Reporting Program (ISMP MERP). High-alert medications top the list of drugs involved in moderate to severe patient outcomes when an error happens.1-2
The Joint Commission has a standard (MM.01.01.03) that requires hospitals to develop their own list of high-alert medications; to have a process for managing high-alert medications; and to implement that process. While most facilities meet the minimum requirements for The Joint Commission (i.e., any list, any process), some hospitals have neither a well-reasoned list of high-alert medications nor a robust set of processes for managing the high-alert medications on their list. Instead, they have a hastily devised list of high-alert medications, which often are not well known to all clinicians, and they may rely on low-leverage risk-reduction strategies to prevent errors, such as staff education and high-alert medication labels on pharmacy bins, to keep patients safe. The hospital may also send memos to staff to increase their awareness of the risks or establish strategies that impact only one aspect of the medication use process—usually drug storage. In some cases, there are no safety nets in place at all, and hospitals are relying on staff vigilance to keep patients safe when receiving high-alert medications. In addition, some hospitals have not updated their list of high-alert medications since it was first mandated by The Joint Commission more than 10 years ago. A list of high-alert medications is relatively useless unless it is up-to-date, known by clinical staff, and accompanied by robust risk-reduction strategies more effective than awareness, manual double-checks, staff education, and appeals to “be careful.” Many of these strategies should be translated for use with other medications.
So, what does it mean if a drug is on your hospital’s high-alert medication list? Does the list serve only to increase awareness of the risk of harm with these medications, or has a robust plan been implemented for each drug or drug class to reduce the risk of errors? Hospitals need a well-thought-out list of specific, high-alert medications and effective high-leverage processes to mitigate the risk of errors with these medications.
Safe Practice Recommendations: We encourage hospitals to take the time to reassess their current list of high-alert medications and any plans that have been enacted to reduce the risk of errors and harm with these drugs. To guide this process, please consider the following:
Develop/Update a Hospital-Specific List
Hospitals need a list of targeted high-alert medications that is comprehensive enough to address the most potentially harmful errors while not being so inclusive that the list is overwhelming. Many hospitals select medications from ISMP’s List of High-Alert Medications, which is updated every few years based on error reports submitted to the ISMP National Medication Errors Reporting Program, reports of harmful errors in the literature, and input from practitioners and safety experts.4 Based on national reports of harm to patients, we believe it is essential for every hospital’s list to include (when used): concentrated electrolytes, neuromuscular blocking agents, opioids (all, not just patient-controlled analgesia), anticoagulants, insulin, epidural or intrathecal medications, and chemotherapy. Other drugs from the ISMP list should be added if use is prevalent or misuse is a concern.
Additional medications to consider for the list may include new drugs added to the formulary, potentially harmful drugs used temporarily during a shortage (which can be removed once the shortage is over), and medications involved in potentially harmful errors based on the hospital’s internal reporting process, even if the drug is not on the ISMP list. For example, after fatal wrong route errors were identified as a potential threat with the new drug EXPAREL (bupivacaine [liposomal] used for local anesthesia into surgical sites) due to its similar appearance to propofol,6 hospitals that added this drug to their formulary should have considered it for addition to their high-alert medication list. Addressing drugs given by a certain route of administration (e.g., intrathecal, epidural) or in special populations (e.g. pediatrics) as high-alert can be effective as well. The hospital’s high-alert medication list should be updated as needed and reviewed at least every 2 years.
Implement Risk-Reduction Strategies
The purpose of identifying high-alert medications is to establish safeguards to reduce the risk of errors with these drugs in all phases of the medication use process. The primary goals of implementing risk-reduction strategies are to: 1) prevent errors, 2) make errors visible, and 3) mitigate harm. To be effective, all of these interdisciplinary components are needed:
Understand the causes of errors. Effective strategies must address the underlying causes of errors with each type of high-alert medication or class of medications. To learn the causes of errors, review internal medication error-reporting data and the results of any applicable root cause analyses. Equally important, a search of the external literature should be completed to uncover reports of errors with high-alert medications that have occurred elsewhere. A failure mode and effects analysis or self-assessment tool also might help identify underlying risks associated with each high-alert medication/class of medications. This important first step should not be skipped—if you can’t describe the ways that errors have happened or could happen with the drug, your strategies may not lessen the risk of an error at all.
Be sure actions are comprehensive. A single risk-reduction strategy for each high-alert medication is rarely enough to prevent harmful errors. The keys to success are as follows:
- Numerous risk-reduction strategies must be layered together to address the targeted risk.
- Risk-reduction strategies should impact as many steps of the medication-use process as feasible given the underlying causes (e.g., procuring, storing, prescribing, transcribing, preparing, dispensing, and administering the medication; monitoring the patient; being prepared for treating [or recovery from] an adverse event if it occurs).
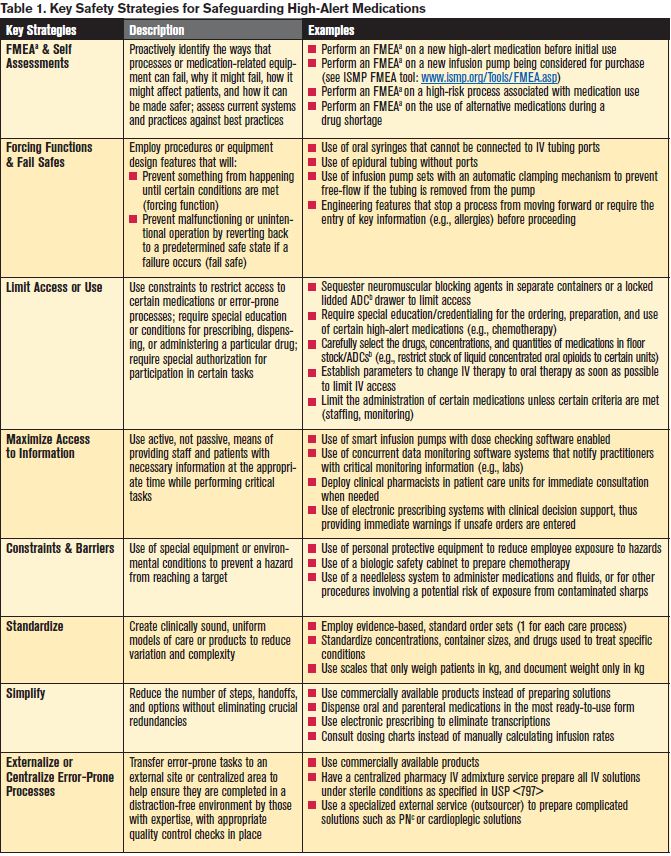
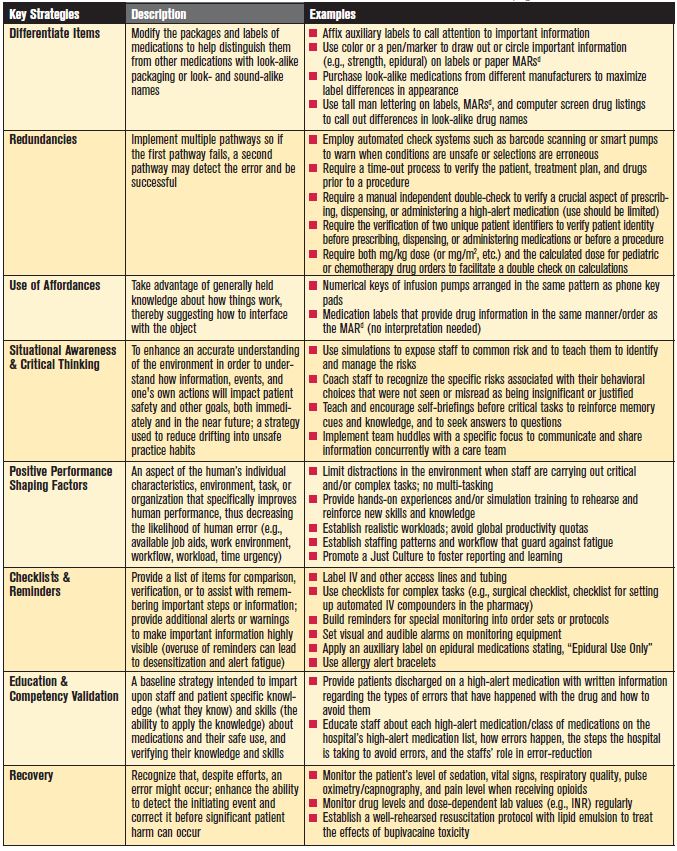
- Low-leverage risk-reduction strategies such as staff education, passive information, and the use of reminders should be bundled together with high-leverage risk-reduction strategies such as forcing functions and fail safes, maximizing access to information, limiting access or use, constraints and barriers, standardization, and simplification. Table 1 provides a description of key risk-reduction strategies listed roughly in descending order of effectiveness based on human factors. We highly encourage hospitals to reference this table whenever risk-reduction plans are being developed.
- To help inform the planning process, the literature should be searched to identify risk-reduction strategies that have been proven effective, recommended by experts, or implemented successfully elsewhere.
- Strategies need to be applicable in various settings.
- When implementing strategies, there must be a balance on how resources will be impacted by the change.
- Strategies must be sustainable over time.
Assess the effectiveness of strategies
Both outcome and process measures should be established and data should be collected routinely to determine the effectiveness of risk-reduction strategies for high-alert medications. The results should be shared regularly in meetings with pharmacy and nursing leadership, the medication safety committee, the pharmacy and therapeutics committee, and other appropriate committees. Reviewing the effectiveness of safeguards and extending the reach of all your risk-reduction strategies are important to ongoing success within your organization.
aFMEA: failure mode and effects analysis bADC: automated dispensing cabinet cPN: parenteral nutrition dMARs: medication administration records
References
- Rickrode GA, Williams-Lowe ME, Rippe JL, et al. Internal reporting system to improve a pharmacy’s medication distribution process. Am J Health-Syst Pharm. 2007;64:1197-202.
- Sakowski J, Newman JM, Dozier K. Severity of medication administration errors detected by bar-code medication administration system. Am J Health-Syst Pharm. 2008;65:1661-6.
- Monroe PS, Heck WD, Lavsa SM. Changes to medication use processes after overdose of U-500 regular insulin. Am J Health-Syst Pharm. 2012;69:2089-93.
- ISMP’s List of High-Alert Medications. 2012.
- National Alert Network. Potential for wrong route errors with Exparel. NAN Alert. March 20, 2012.
- Cohen MR, Smetzer JL, Tuohy NR, et al. High-alert medications: safeguarding against errors. In: Medication Errors. Cohen MR ed.; Washington, DC: The American Pharmacist Association. 2007;317-412.