
Two New Best Practices in the 2020-2021 Targeted Medication Safety Best Practices for Hospitals
ISMP has released its 2020-2021 Targeted Medication Safety Best Practices for Hospitals. The purpose of the Targeted Medication Safety Best Practices is to identify, inspire, and mobilize widespread, national adoption of consensus-based Best Practices to address recurring problems that continue to cause fatal and harmful errors despite repeated warnings in ISMP publications. The Best Practices, which are reviewed by an external expert advisory panel and approved by the ISMP Board of Trustees, are designed to be realistic and have already been successfully adopted by numerous organizations. Equally important, their implementation can vastly improve medication safety and reduce the risk of significant patient harm.
Two New Best Practices for 2020-2021
First introduced in 2014 with 6 Best Practices, the Targeted Medication Safety Best Practices for Hospitals are reviewed and updated every 2 years. The 2020-2021 list now comprises 16 Best Practices, including 2 new ones described below:
New Best Practice 15: Opioid Prescribing
Verify and document a patient’s opioid status (naïve versus tolerant) and type of pain (acute versus chronic) before prescribing and dispensing extended-release and long-acting opioids.
-
Default order entry systems to the lowest initial starting dose and frequency when initiating orders for extended-release and long-acting opioids.
-
Alert practitioners when extended-release and long-acting opioid dose adjustments are required due to age, renal or liver impairment, or when patients are prescribed other sedating medications.
-
Eliminate the prescribing of fentaNYL patches for opioid-naïve patients and/or patients with acute pain.
-
Eliminate the storage of fentaNYL patches in automated dispensing cabinets (ADCs) or as unit stock in clinical locations where acute pain is primarily treated (e.g., in the emergency department [ED], operating room, postanesthesia care unit, procedural areas).
Best Practice 15 has replaced Best Practice 12, which focused solely on eliminating the prescribing of fentaNYL patches for opioid-naïve patients and/or acute pain, and eliminating the storage of fentaNYL patches in areas where acute pain is primarily treated.
New Best Practice 16: ADC “Override” Feature
a) Limit the variety of medications that can be removed from an ADC using the override function.
b) Require a medication order (e.g., electronic, written, telephone, verbal) prior to removing any medication from an ADC, including those removed using the override function.
c) Monitor ADC overrides to verify appropriateness, transcription of orders, and documentation of administration.
d) Periodically review for appropriateness the list of medications available using the override function.
- Restrict medications available using override to those that would be needed emergently (as defined by the organization) such as antidotes, rescue and reversal agents, life-sustaining drugs, and comfort measure medications such as those used to manage acute pain or intractable nausea and vomiting.
Survey to Measure Baseline Implementation of New Best Practices
ISMP is conducting a short survey to get a sense of the baseline level of implementation of these 2 new Best Practices. We would appreciate your participation in this survey regardless of whether you have implemented the Best Practices. Please complete the survey online by April 17, 2020. The survey questions are provided on page 6, in the PDF version, for your review prior to taking the online survey.
Other Changes for 2020-2021
Five of the 2018-2019 Best Practices were revised or archived in 2020 (changes displayed in bold, underlined font, when appropriate):
Best Practice 4: Pharmacy Dispensing in Oral/Enteral Syringes
Ensure that all oral liquid medications that are not commercially available in unit dose packaging are dispensed by the pharmacy in an oral syringe or an enteral syringe that meets the International Organization for Standardization (ISO) 80369 standard, such as ENFit. (Previously, the Best Practice called for pharmacy to dispense oral liquid medications in an “oral or ENFit syringe.” The change was made should another ISO-compliant product become available.)
Best Practice 5: Dosing Devices that Measure Only in Metric Scale
Purchase oral liquid dosing devices (oral syringes/cups/droppers) that only display the metric scale. In addition, if patients are taking an oral liquid medication after discharge, educate patients to request appropriate oral dosing devices to measure oral liquid volumes in milliliters (mL) only. (Previously, the Best Practice recommended supplying patients “with [or provide a prescription for] oral syringes, to enable them to measure oral liquid volumes in milliliters [mL].” The change was made because not all patients need a prescription, and the measuring device should only measure in mL.)
Best Practice 6: Glacial Acetic Acid
Eliminate glacial acetic acid from all areas of the hospital. (This Best Practice was archived because hospitals have shown progress in removing or replacing it with vinegar or commercially available diluted acetic acid to prevent accidental use.)
Best Practice 8: Programmable Infusion Pumps with DERS
a) Administer medication infusions via a programmable infusion pump utilizing dose error-reduction systems (DERS). (Previously, this Best Practice recommended administering “high-alert IV medication infusions” via programmable infusion pumps with DERS. The change was made to broaden the scope to all medication infusions. New elements [b, c, d, and bullet points—next page] added a metric component, reconciliation between the library and electronic health records [EHRs], and planning for interoperability.)
NEW b) Maintain a 95% or greater compliance rate for the use of DERS.
NEW c) Monitor compliance with use of smart pump DERS on a monthly basis.
NEW d) If your organization allows for the administration of an IV bolus or a loading dose from a continuous medication infusion, use a smart pump that allows programming of the bolus (or loading dose) and continuous infusion rate with separate limits for each.
-
Allocate resources for ongoing maintenance, updating, and testing of the software and drug library for all smart infusion pumps.
-
Ensure drug library content is consistent with the drug information and nomenclature (e.g., drug name, dosing units, dosing rate) in the EHR.
-
Plan for the implementation of bi-directional (i.e., auto-programming and auto-documentation) smart infusion pump interoperability with the electronic health record.
Best Practice 11: Ingredient Verification Prior to Mixing
When compounding sterile preparations, perform an independent verification to ensure that the proper ingredients (medications and diluents) are added, including confirmation of the proper amount (volume) of each ingredient prior to its addition to the final container.
REMOVED: At a minimum, perform this verification for all high-alert medications (including chemotherapy and parenteral nutrition), pediatric/neonatal preparations, pharmacy-prepared source/bulk containers, products administered via high-risk routes of administration (e.g., intrathecal, epidural, intraocular), and other compounded sterile preparations that the organization believes are high-risk. (This bullet point was removed to broaden the scope of this Best Practice to all compounded sterile preparations.)
Prior Survey Results
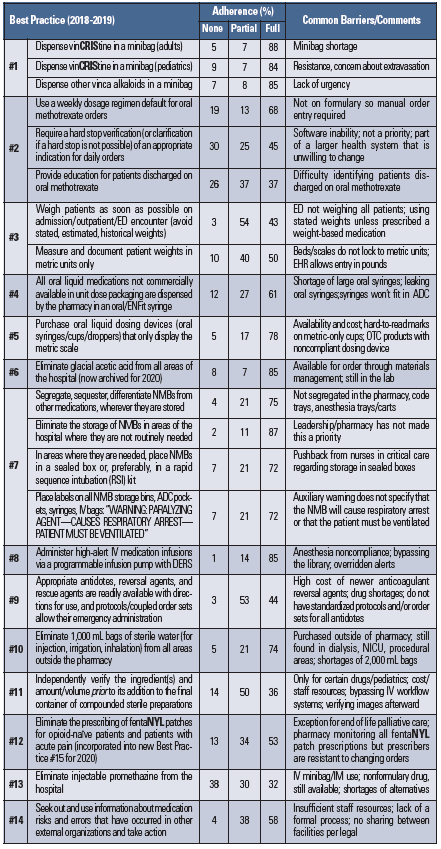
Prior to releasing the 2020-2021 Targeted Medication Safety Best Practices for Hospitals, ISMP conducted a survey between June and July 2019 to measure progress with implementing the existing 2018-2019 Best Practices. These results were presented at the American Society of Health-System Pharmacists (ASHP) Midyear Clinical Meeting on December 11, 2019. In case you missed that presentation, we have provided an overview of the survey findings in Table 1. Most of the 347 survey respondents were from large US hospitals with more than 100 beds (78%). Approximately half of all hospitals had one or more full- or part-time medication safety officer(s) (MSO[s]). Hospitals with an MSO tended to report full compliance with the Best Practices more frequently than hospitals without an MSO, with one exception. Eliminating injectable promethazine from the hospital, Best Practice #13, has been fully implemented (36%) in hospitals WITHOUT an MSO more frequently than in hospitals with an MSO (28%).
Table 1. Adherence with 2018-2019 Targeted Medication Safety Best Practices for Hospitals (N=347)
Conclusion
Hospitals and health systems should focus their medication safety efforts over the next 2 years on these 2020-2021 Best Practices. The rationale for recommending the Best Practices, along with related ISMP publications and guidelines for additional information, can be found in the full document. Related documents that might be helpful to hospitals include Frequently Asked Questions (FAQs) and an Implementation Worksheet. Also, please don’t forget to complete our short survey on the 2 new Best Practices for 2020-2021.
Access this Free Resource
You must be logged in to view and download this document.