Survey on LASA Drug Name Pairs: Who Knows What's on Your List and the Best Ways to Prevent Mix-Ups?
Not a week goes by that we don’t hear about mix-ups between two products with similar names. Too many of these mix-ups have led to harmful or fatal medication errors. Increasingly, pharmaceutical manufacturers and regulatory authorities have been taking measures to determine if there are unacceptable similarities between proposed names and products on the market. Some improvement has occurred in recent years, but factors such as handwritten and verbal prescriptions—which can easily be mistaken as look-alike or sound-alike (LASA) drug names—and the vast number of different products on the market have impeded full resolution of the problem.
In March 2009, we distributed a subscriber survey to learn how healthcare providers are dealing with LASA drug names. This safety problem has been the focus of one of The Joint Commission’s (TJC) National Patient Safety Goals (NPSGs) since 2005. The NPSG requires accredited organizations to maintain and annually review a list of at least 10 LASA name pairs, and to take action to prevent the interchange of these products. Surprisingly, our survey found that more than a quarter of responding nurses did not know whether their organizations maintained a list of LASA drug names. Almost 850 people—mostly nurses (371) and pharmacists (285)—responded to our survey, and here’s what else they had to say.
List of LASA drug name pairs
About 80% of respondents reported that their organization maintains a list of LASA drug name pairs that could be confused with each other. Uncertainty about whether their organization maintains such a list was greater among staff nurses (27% uncertain) than staff pharmacists (3% uncertain). About a quarter (26%) of respondents felt they could name most of the drug name pairs on their organization’s list; 5% could not name any drugs on their LASA list.
Half of respondents’ LASA list contained more than 15 name pairs; 30% contained 11-15 name pairs; 14% included 10 name pairs; and 6% contained less than 10, the minimum number required by TJC NPSG. The most common resources used to select the name pairs on the list included: TJC LASA list (48%), ISMP LASA list (35%), and internal staff reports (32%). However, 39% of staff nurses and 16% of staff pharmacists had no idea where the list originated. Half of respondents (54%) reported adding new drug name pairs to the initial list compiled in their organization, but almost a third (29%) of respondents were uncertain whether any drug name pairs had ever been added.
Risk-reduction steps
Among respondents with a list of LASA drug name pairs, 87% reported that their organizations have identified risk-reduction steps to reduce confusion between these drugs. Of those, only half felt their organization had implemented all the identified risk-reduction steps. About 11% of respondents were uncertain whether their organization had identified and/or implemented any risk-reduction steps; 2% said no steps have been identified or implemented.
The most common resources used to identify risk-reduction steps included best practice recommendations in the literature (41%), ISMP resources (38%), and analysis of internal medication-use systems (37%). The risk-reduction steps most frequently addressed drug dispensing processes (91%), drug storage (89%), and drug administration (80%). Least frequently addressed steps included drug procurement procedures (57%), transcription of drug orders (60%), and prescribing (65%).
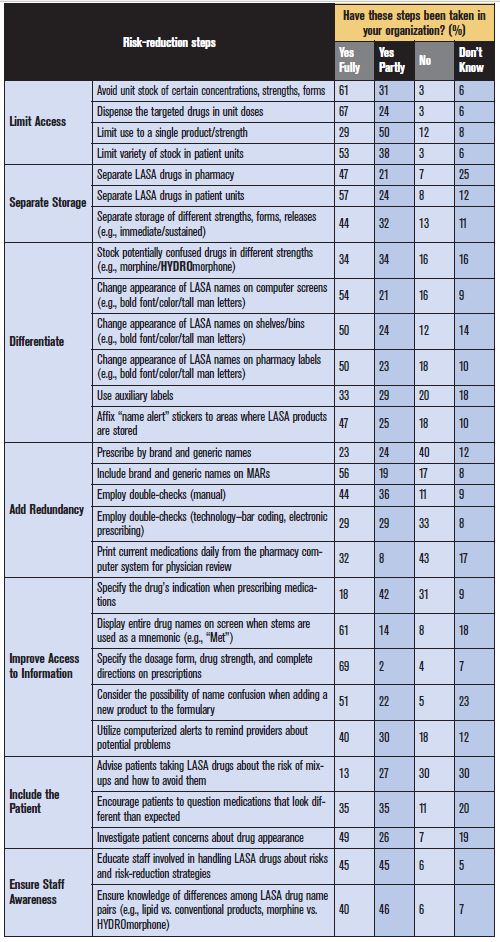
Table 1 lists specific risk-reduction strategies and how frequently they were reported as being employed by respondents. The most frequently implemented risk-reduction steps involved limiting access to drugs on the LASA list, particularly avoiding unit stock and instead dispensing the prescribed products from the pharmacy in unit doses. Displaying the entire drug name on computer screens when stems are used for mnemonics, and requiring prescribers to include the dosage form, strength, and complete instructions also ranked among the top risk-reduction strategies. Risk-reduction steps that involved patients—such as investigating their concerns about drug appearance—were the least frequently employed group of strategies, as were redundancies, particularly prescribing by brand and generic names, bar-coding, and daily physician review of currently prescribed drugs. Including the drug’s indication when prescribing medications also scored low, with only a few respondents employing this strategy. Not listed as a choice on our survey, automated dispensing cabinets were mentioned by some respondents as one means of decreasing mix-ups if the LASA drugs are stored in separate drawers that open only when selected, and if the LASA drug names are easily distinguishable on the screen.
Effectiveness of risk-reduction steps
On average, about 82% of all respondents believe the risk-reduction strategies taken in their organization to guard against confusion with LASA drug name pairs have been effective. However, pharmacists (86%) were more likely to believe this than nurses (76%). Importantly, about three-quarters of staff nurses (76%) and pharmacists (78%) agreed that the strategies taken by their organizations to guard against confusion had actually prevented them from making a mistake with the targeted LASA drugs.
Conclusions
Compliance rates with TJC NPSG for LASA drugs have been high: at least 90% in all types of organizations and 95% in 2008 for hospitals. Yet, our survey suggests that more can be done to reduce the risk of errors with LASA drugs. The first point of business: All clinical staff involved in medication use, particularly frontline nurses, pharmacists, physicians, unit secretaries, and technicians, need to be aware of the organization’s list of LASA products, how it was selected and is updated, what it means, why it is important to patient safety, and the steps laid out to reduce mix-ups.
Keeping the list manageable is also crucial. A manageable number of drug name pairs on the list should not prevent you from taking steps—from bar-coding technology to the use of tall man letters when appropriate—to reduce mix-ups among many different products with LASA names. However, the targeted LASA list maintained in your organization should serve to draw special attention to a finite number of products that can cause great harm if confused, and to promote knowledge of and compliance with drug-specific risk-reduction strategies. Further, when adding a new name pair to the list, an awareness campaign is needed. In addition, don’t forget to employ risk-reduction strategies that target the procurement, transcription, and prescribing of the drug name pairs on your LASA list, and to expand the patient’s role to help ensure a mix-up does not happen—all areas our survey suggested are often overlooked.
TJC is currently seeking comments on proposed changes to the NPSGs. For LASA drug names, TJC plans to move this NPSG to the Medication Management standards. The standard will still require an annually reviewed list of LASA medications, but the minimum number of drug name pairs is no longer specified. The proposed elements of performance state that the LASA list must be based on a review of the LASA medications published by ISMP. As in the current NPSG, organizations are required to take action to prevent errors involving the interchange of the products on the list.
We thank all 842 respondents who participated in our survey. We appreciate responses from clinical staff who admitted little or no knowledge about their organization’s LASA list. We also appreciate the insightful comments participants added to the survey. As with our other surveys, we learned from your responses, which can be used to strengthen our understanding and recommendations regarding LASA drugs.