
Safety Brief: Generic EPINEPHrine autoinjectors
EPINEPHrine is dosed by weight when used to treat an allergic reaction or anaphylaxis, not by whether the patient is an adult or child. Thus, generic brands of the EPINEPHrine autoinjector do not use the abbreviation “Jr” for the 0.15 mg dosage strength (see Figure 1).
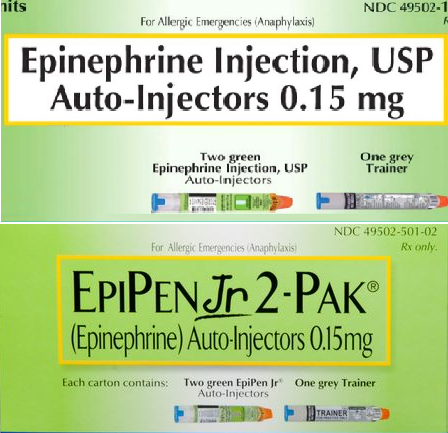
The abbreviation “Jr” is already part of the EPIPEN trademark used for that strength. However, given that dosing is weight-based, please be sure staff are aware that generics will list the metric strength only, 0.3 mg or 0.15 mg. Patients 30 kg (approximately 66 pounds) or heavier should use a 0.3 mg injector. Those who weigh between 15 to 30 kg (33 pounds to 66 pounds) need to use a 0.15 mg injector. Both strengths should be available for treatment in healthcare facilities. A pharmacist expressed concern that practitioners unfamiliar with EPINEPHrine dosing may confuse the strengths if they are accustomed to seeing the “Jr” designation.
Simulation products look real. Medications used for educating healthcare practitioners during simulation exercises, also known as demo medications, often appear very similar to the actual medication. The names on some simulation products contain the same letters as the real drug name with a few characters left out, as in the case of “AUGMENTN” (see Figure 2), an example we recently encountered. Practitioners often look at labels and read only the first few letters before their brain decides what the label says. This is an example of confirmation bias, which leads individuals to “see” information that confirms their expectations, rather than information that contradicts their expectations. Once the first few letters in a drug name are confirmed, a practitioner may not recognize the subtle differences between the simulation and actual product, even with careful inspection.

Simulation products may also bear the actual product name. Some even contain a fluid vehicle such as 0.9% sodium chloride. However, because they are produced for training purposes only, they are nonsterile and not meant for patient use.
We first described a mix-up between an actual and a simulation product in our November 28, 2013 newsletter, where a carton of “Epinephrn” was placed in a crash cart instead of actual EPINEPHrine. In an emergency, a practitioner could have failed to notice that it was a simulation product. In 2015, we learned from the US Food and Drug Administration (FDA) that more than 40 patients were administered a simulated intravenous (IV) fluid and developed adverse reactions including fever, tremors, and chills. This led to hospitalization for some and, in one instance, death (www.ismp.org/node/552). FDA (www.ismp.org/ext/113) and the Centers for Disease Control and Prevention (CDC) (www.ismp.org/ext/114) have also warned about simulated medications.
As the above incidents have shown, steps must be taken to ensure that simulation products do not enter the supply chain, where they could be used in real patient care situations. Simulation products should only be stored in non-patient care areas such as classrooms and other educational simulation areas. Instructors should account for each demo product at the end of class to ensure they do not travel outside the room in someone’s pocket. Alert healthcare practitioners to the nearly identical product labeling often used on these products and their proper use and storage.