
Product-Related Issues Make Error Potential Enormous with Investigational Drugs
Problem: Routine practices used to name, label, package, and store investigational drugs raise serious patient safety concerns. Just last week, a pharmacist sent us an example that illustrates several error-prone aspects of the labeling of investigational drugs. In a Bristol-Myers Squibb investigational study comparing apixiban and enoxaparin, the packaging of the enoxaparin and placebo syringes is of concern. The plain-looking syringes are labeled with an identification number. The syringe labels do not include lot numbers or expiration dates. The most predominant feature on the syringes is the company name. Although syringes are provided in a labeled carton, once the syringes are removed from the box, the carton label containing important information is lost. 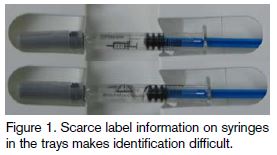 One can see how easy it would be for patients assigned to the study drug group or the placebo group to receive medication from the wrong syringe once the products are sent to a patient care unit (see Figure 1). Similarly, apixiban tablets are provided in bulk supplies, not unit-dose packages, adding to the potential for inaccurate doses.
One can see how easy it would be for patients assigned to the study drug group or the placebo group to receive medication from the wrong syringe once the products are sent to a patient care unit (see Figure 1). Similarly, apixiban tablets are provided in bulk supplies, not unit-dose packages, adding to the potential for inaccurate doses.
According to numerous pharmacists who have provided information to ISMP, many other safety concerns exist with investigational drugs:
Drug names. Investigational drugs are most often identified using a number preceded by an abbreviation of the sponsoring company’s name (e.g., BMS104579 for a drug sponsored by Bristol-Myers Squibb)—much like a vehicle license plate. Many organizations that participate in investigational drug studies are involved in multiple studies by the same sponsor; thus, the sponsor’s abbreviation preceding the identification number adds to the similarity of the investigational drug identification schema. Some letter/number designations are up to 25 characters long, or are described with multiple words, forcing pharmacy computer systems to truncate the code name due to field size limitations. Many blinded studies employ placebo drugs, so the product number needs to be clearly visualized and confirmed to ensure the patient gets the correct medication and dose. Yet, identifying the products is often a challenge due to the sponsor’s naming schema. During the life of a study, a product with a license plate-type code name may get a generic or common name. In many cases, the code name remains on the product label, but the research team often refers to the drug by its new generic name. It is even possible for the code name to change, particularly if the sponsor is part of a merger or the company or product is sold.
Drug labels. Many investigational drugs are labeled using a very small font size; in most cases, a magnifying glass is needed to read the information (see Figure 2). 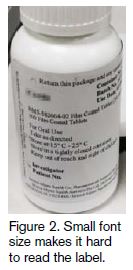 The same font size is often used throughout the label, and there is little use of bold type, color, tall-man letters, or other strategies to help differentiate products. Thus, drug packages look remarkably similar, which can lead to confirmation bias when products are selected from the shelf. The labels may not include the drug strength or concentration, even if there are multiple drug strengths/concentrations in use. If the drug is involved in an international study, the directions may be printed in two or more languages on the same label. Labels may also include error-prone abbreviations or dose designations (e.g., 5IU, which looks like 51 Units, or trailing zeros [1.0 mg]).
The same font size is often used throughout the label, and there is little use of bold type, color, tall-man letters, or other strategies to help differentiate products. Thus, drug packages look remarkably similar, which can lead to confirmation bias when products are selected from the shelf. The labels may not include the drug strength or concentration, even if there are multiple drug strengths/concentrations in use. If the drug is involved in an international study, the directions may be printed in two or more languages on the same label. Labels may also include error-prone abbreviations or dose designations (e.g., 5IU, which looks like 51 Units, or trailing zeros [1.0 mg]).
Drug packaging. Many oral investigational drugs are not supplied in unit-dose packages. Additionally, vial sizes of parenteral drugs are sometimes inappropriate for the dose being studied and may require dozens of vials to prepare a single dose. This sensitizes practitioners to expect to use many vials when preparing a dose of the medication. Thus, recognition of a possible overdose is less apparent during the preparation of investigational drugs than it would be during preparation of other drugs, where the use of dozens of vials for a single dose would clearly signal an error.
Tablet markings. Multiple strengths of tablets often look identical in color and size, and they have no markings to help differentiate the strengths. While this may be essential for blinded studies (in which the strength is not known to the patient, provider, and at times, the research team), the same batches of look-alike tablets may be used for open label studies as well (where the tablet strength is known to all).
Expiration dates. Because “beyond use” dates of investigational drugs may be updated during a trial based on ongoing testing, some sponsors do not list an expiration date on the product package, or even on a packing slip or receipt. Instead, the sponsors require participating organizations to call an interactive voice response system (IVRS) to check expiration dates—a process that is time consuming. Lag time with the IVRS has resulted in cases where expired drugs have not been replaced in time, or direct intervention with the sponsor was needed to avoid dispensing a drug that would reach expiration during outpatient use.
Space limitations. Investigational drugs require separate, dedicated storage space. However, as new protocols are added to a research organization’s therapies, the storage space allotted for investigational drugs can quickly become exhausted. Also, pharmacy space is often occupied storing investigational drugs that are awaiting pick-up and disposal by the sponsor. Some smaller facilities have stored investigational drugs in the office of a research pharmacist or nurse. Space limitations lead to crowded shelves and other unsafe storage conditions, increasing the risk of choosing the wrong look-alike investigational drug.
Reporting errors. Similar to an adverse reaction, when an error happens with an investigational drug, it must be reported to the drug sponsor and the organization’s Institutional Review Board (IRB). The error is also reported through an organization’s internal reporting system and investigated in the same manner as other serious errors. The Principal Investigator (PI) from within the organization and a study monitor who is responsible for following the investigational drug protocol at multiple sites will usually determine whether the error should also be classified as a study deviation/violation, then report the information to the sponsor. The affected patient is often excluded from the study, and at times, the site where the error occurred may be excluded from the study. Yet, any system-based causes of the error under the direct control of the sponsor—that is, naming, labeling, and/or packaging of the drug—are rarely addressed or remedied. Once an error has been reported to the drug’s sponsor, it is unclear whether it is, or must be, reported to FDA. Our sources suggest that adverse reactions are more likely to be reported to FDA than actual errors.
Risk of errors not considered. While the error-prone conditions listed above may be readily apparent to practicing healthcare providers, scientists working on new drug development, product manufacturing, and protocols for clinical trials are rarely well versed in basic medication safety principles. They often have little or no recent practical experience prescribing, dispensing, or administering medications. The sponsoring company’s attention tends to be on the safety profile of the drug and its clinical effects on patients; adherence to safe labeling and packaging practices is a low priority. This also seems to be the case when outside companies run the clinical trials for the sponsors. Additionally, there appears to be little regulatory oversight governing the labeling, packaging, and nomenclature used to identify investigational drugs.
Safe Practice Recommendations
The risks related to medication errors with investigational drugs are not easily remedied since many problems stem from the way the drugs are named, labeled, and packaged by the sponsor. To that end, ISMP hopes to obtain funding to hold a summit in 2008 with industry leaders to explore problems and propose solutions. Meanwhile, there are several steps that organizations can take to reduce the risk of medication errors when using investigational drugs.
Promote safe storage. Provide adequate space to stock investigational drugs, away from other medications. Organizations that participate in many studies often have a separate pharmacy for investigational drugs. Pharmacies often separate investigational drugs in bins labeled with their associated IRB numbers, since the drugs are often prescribed according to the IRB number. Consider drug storage when reviewing new protocols submitted for IRB approval, and address any concerns before participating in the study. Notify sponsors that unneeded study medications and supplies will be discarded by a specific date if not picked up before then. If possible, consider moving unneeded supplies to a secure, locked space outside the pharmacy until retrieval.
Highlight information. A pharmacy-prepared auxiliary label can be affixed to individual drugs or a bag that holds a supply of vials/containers of the same drug/strength/concentration. These labels should supply information that is missing on the product label (e.g., strength, concentration, lot numbers), or information that is poorly visible on the label. You can also use colored highlighter pens or black sharpie pens to bring attention to key information on the label, mark the identification code on top of each kit/bottle top, or rewrite the mg strength on an empty portion of the label. Auxiliary labels and highlights should be applied before the drugs are added to stock or dispensed to patient care areas. In some cases it might be appropriate to repackage the medication in unit doses before dispensing to patient care areas, unless the characteristics/stability of the drug make this impossible or the research protocol disallows it.
Enhance prescription labeling. Sponsors usually do not allow investigational drugs to be transferred out of the original container. Thus, when dispensing an investigational drug to a patient, the pharmacy should provide a supplemental label that meets all standards for prescription dispensing that are applicable in the state. Flagging or folding the label might be necessary to avoid covering information on the original container.
Educate sponsors. Perform a risk assessment on new investigational drugs and communicate the safety issues related to medication errors to the sponsor during the study initiation meeting. Recognize that you may be providing information about the risk of medication errors to a sponsor representative who has never considered these issues. Although it is unlikely that immediate changes will be made based on safety concerns you express, consistent feedback to sponsors about medication safety issues may result in safer product naming, packaging, and labeling in future studies.
Assess error potential during IRB review. An organization’s IRB should include membership by pharmacists, and investigational drug protocols and other issues related to medications should be assessed for safety (e.g., proper labeling) and considered by the IRB before approval is granted. If drug labeling and packaging information has not been provided with the protocol, request information from the sponsor to help facilitate evaluation.
Report errors. Continue to report errors to the IRB and study sponsor. ISMP also urges organizations to report errors with investigational drugs to the USP-ISMP Medication Errors Reporting Program (or write to [email protected]). These reports will then be shared with USP and FDA. (The reporter’s identify is redacted if requested.) By learning more about these errors, patient safety advocates can work with sponsors in the pharmaceutical industry to spur necessary changes. Appropriate agencies within The National Institutes of Health (NHI) (e.g., National Cancer Institute) also should be notified of errors so they can monitor clinical trials appropriately.