
Preventing Medication Errors During Codes
Problem: Cardiac and/or respiratory resuscitation is an extremely stressful situation during which healthcare practitioners have little time for discussion and verification of the patient’s treatment plan, including medications. During these medical emergencies—often referred to as a code blue—every second counts and every errant action or inaction can result in patient harm or death. While studies regarding medication errors during codes1-3 have documented variable incidence rates—from less than 1%1 when studying reported events to 15%2 from observations during simulations—two facts are clear:
- Patient harm from medication errors during code conditions is high1-5
- Serious errors are often missed, even if the patient died or is harmed, because there was no suspicion that the drugs actually caused or contributed to the morbidity or mortality.2-3
For example, one study documented that medication errors during codes are 39 times more likely to result in harm and 51 times more likely to result in death than non-code related medication errors.1 This finding is not surprising because many of the drugs administered during a code are high-alert medications, and patients are at their most vulnerable state during medical emergencies. In another study, researchers who analyzed the actual drug content in syringes used during code simulations found substantial deviations from the expected dose in 16% of the syringes, suggesting that unrecognized medication errors may be a major source of morbidity and mortality in resuscitated patients, including children.2
The types of errors that occur during codes are varied. However, numerous studies have suggested that the most common types of errors occurring during codes are: dosing errors, drug selection errors, drug preparation errors, administration technique errors, and omissions.1-5 About a quarter of these errors originate during dispensing/preparation of the drug; about half originate during administration of the medication; and about 10% occur during the prescribing process.1 In addition, a study of mock pediatric resuscitations showed that approximately one in five verbal orders did not specify an exact dose, and about half did not include the route of administration.2 The wrong dose prescribing errors that occurred during this study2 included 10-fold overdoses, total daily doses ordered as a single dose, and ordering the wrong concentration of dextrose for an infant. Furthermore, about 12% of the ordered drugs in this study were never administered.
Examples of actual errors that have been reported to the ISMP Medication Errors Reporting Program or errors published in the referenced journal articles are provided in Table 1.
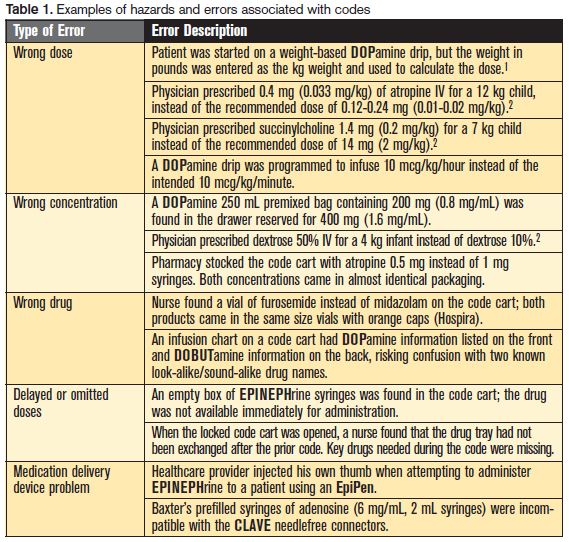
Most often, these errors involve reliance on human calculations, miscommunication, protocol deviation, knowledge deficit, or a dispensing device problem. Commonly reported contributing factors include: look-alike product packaging or drug names; disorganized and nonstandard code carts; excessive stock in code carts; distractions caused by the hectic environment; poorly communicated verbal orders; inexperienced staff; alternative drugs in code carts during a drug shortage; confusing or missing information about drugs; and multiple concentrations of a drug in code cart drawers.
A study published in 2008 also points out that patients involved in codes are not the only ones who may be affected by medication errors during the code.1 Other patients assigned to staff who attend the code may be victims of errors—called “collateral damage” by the study authors. These medication errors, which were rarely harmful, were mostly missed respiratory therapy treatments that were supposed to be administered by respiratory therapists who were busy attending a code.
Safe Practice Recommendations
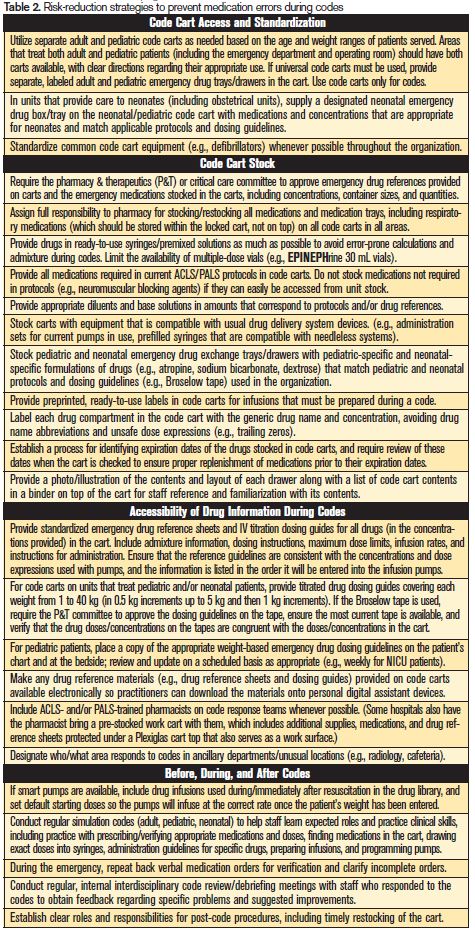
Ideally, reducing the incidence of emergency resuscitations would simultaneously reduce the incidence of errors during codes. Interventions such as ensuring adequate patient-to-staff ratios for appropriate monitoring and the ability to activate rapid response teams to address ongoing concerns with the patient’s condition before it deteriorates into a code situation can help in this regard. However, there will always be unstable patients who are vulnerable to codes, and patients who arrive at the hospital in full cardiac and/or respiratory arrest. Thus, organizations need to address medication error risks that may be present during these unique and often chaotic situations. One study1 that examined medication errors associated with codes showed that action to reduce the risk of similar errors was documented for only 29% of the errors. When action was taken, the most common strategies were to inform staff who made the error and provide additional education—both low leverage strategies. Less than 5% of the errors resulted in system- or policy-level action. Table 2 provides a list of strategies to decrease the risk of medication errors during codes. The list can be used to assess current practices and establish an action plan with high-leverage strategies that are more likely to reduce the risk of errors during codes.
References
- Lipshutz AKM, Morlock LL, Shore AD, et al. Medication errors associated with code situations in US hospitals: direct and collateral damage. Joint Com J on Qual and Pt Safety. 2008;34(1):46-55.
- Kozer E, Seto W, Verjee A, et al. Prospective observational study on the incidence of medication errors during simulated resuscitation in a paediatric emergency department. BMJ. 2004;329:1321.
- Strzyzewski N. Common errors made in resuscitation of respiratory and cardiac arrest. Plast Surg Nurs. 2006;26:10-14.
- Kozer E, Scolinik D, Macpherson A, et al. Variables associated with medication errors in paediatric emergency medicine. Paediatrics. 2001;110:737-42.
- Hunziker S, Tschan F, Semmer NK, et al. Human factors in resuscitation: lessons learned from simulator studies. J Emerg Trauma Shock. 2010;3(4):389–394.