
Prevent Errors During Emergency Use of Hypertonic Sodium Chloride Solutions
Problem: As early as 1919, hyperosmolar agents administered intravenously (IV) were shown to reduce intracranial pressure (ICP) or reduce cerebral edema in adult and pediatric patients after neurological injury, including traumatic brain injury (TBI), subarachnoid hemorrhage (SAH), acute ischemic stroke (AIS), intracerebral hemorrhage (ICH), and hepatic encephalopathy (HE).1-3 The hyperosmolar therapy reduces ICP by establishing an osmotic gradient between the extracellular and intracellular space, thereby optimizing blood viscosity and cerebral blood flow. Mannitol as a hyperosmolar agent was introduced in 1961 and became the agent of choice to manage ICP.1,4 In the 1990s, hypertonic sodium chloride (e.g., 3%, 5%, 23.4%) was introduced as a hyperosmolar agent, and its use to manage ICP has increased while mannitol use has decreased.1,5
Using hypertonic sodium chloride rather than mannitol has become the standard of care in treating several neurological injuries. For adults, current guidelines suggest the use of hypertonic sodium chloride over mannitol for the management of elevated ICP or cerebral edema in patients with TBI or ICH, and for patients with AIS who do not respond adequately to mannitol.3 For other neurological injuries, using either mannitol or hypertonic sodium chloride is recommended. For pediatric patients 18 years and younger with a severe TBI, current guidelines suggest using hypertonic sodium chloride.1 Mannitol has not been subjected to current controlled clinical trials in children—most investigations were carried out in both children and adults in the 1970s.1,4 For refractory ICP and cerebral herniation syndrome, 23.4% sodium chloride is recommended for both adult and pediatric patients.1,3
Hypertonic sodium chloride has several theoretical advantages over mannitol, including 1) less penetration of sodium across the blood-brain barrier, 2) lack of a diuretic effect, 3) restoration of normal cellular resting membrane potential and cell volume, 4) stimulation of arterial natriuretic peptide release, 5) inhibition of inflammation, and 6) enhancement of cardiac output.1,3 Once administered, hypertonic sodium chloride begins to reduce ICP within minutes; its peak is at 20-30 minutes; and ICP reduction lasts for 6-24 hours.
Recent Errors
Since the beginning of 2020, most errors associated with hypertonic sodium chloride reported to the ISMP National Medication Errors Reporting Program (ISMP MERP) occurred during preparation in the pharmacy. For example, there were numerous errors in which the wrong concentration of sodium chloride was used to manually compound a solution or was loaded incorrectly onto an auto-compounder, and 23.4% sodium chloride vials were used instead of sterile water to compound parenteral fluids for neonates. These errors were often associated with look-alike labeling and packaging of the products. A few reports were associated with prescribing errors in which physicians ordered the wrong sodium chloride concentration to be added to compounded IV solutions for pediatric patients with an elevated ICP. These errors were often caused by a confusing prescribing process or unfamiliarity with the solutions used to treat elevated ICP.
We received a few reports about stocking/storage errors (e.g., 500 mL bags of 3% sodium chloride stocked instead of 0.9% sodium chloride or look-alike magnesium sulfate 20 g/500 mL bags). In one report, the central supply department distributed 500 mL bags of 3% sodium chloride instead of 0.9% sodium chloride to various patient care units. We also received numerous drug administration error reports. A few involved mix-ups between 500 mL bags of 3% sodium chloride and either 0.9% sodium chloride or 5% dextrose in 0.3% sodium chloride when retrieving IV solutions from an automated dispensing cabinet (ADC). Intravenous administration errors also involved infusing 3% sodium chloride solution longer than prescribed, and administering the solution at 100 mL/hour instead of 25 mL/hour.
We also learned about dosing errors that occur during order entry or when programming smart infusion pumps because pediatric hypertonic sodium chloride may be dosed in mEq/kg, mEq/kg/hour, mL/kg, or mL/kg/hour. In fact, when providers verbally order repeat doses of hypertonic sodium chloride at the child’s bedside, the dose is often expressed in mL/kg (as noted in prescribing information and dosing guidelines1,3) or mL/kg/hour, but the smart infusion pump libraries may list the solution in mEq/kg (bolus dose) or mEq/kg/hour (infusion).
Delays in Treatment
In a March 25, 2021, Medication Safety Officers Society (MSOS) Briefing, we heard from several facilities with a high demand for hypertonic sodium chloride to treat elevated ICP that were struggling with clinical delays in treatment while awaiting pharmacy preparation and dispensing of all doses or infusions. ISMP’s 2019 Guidelines for the Safe Use of Automated Dispensing Cabinets recommend to avoid stocking vials/ampules of concentrated electrolytes, including sodium chloride in concentrations greater than 0.9%, in ADCs. A Frequently Asked Question (FAQ) associated with this guideline specifically notes that vials of 23.4% sodium chloride should not be stocked in ADCs, suggesting that the pharmacy should prepare, label with appropriate warnings, and hand-deliver any IV push doses of 23.4% sodium chloride used in critical care or emergency/urgent care units.
Our 2017 ISMP Medication Safety Self Assessment® for High-Alert Medications provides the same recommendations for vials/ampules of 23.4% sodium chloride, but also suggests that appropriately labeled and sequestered bags of 3% sodium chloride may be stocked in limited quantities in approved critical care or emergency/urgent care units. Nevertheless, since hypertonic sodium chloride, especially 23.4% sodium chloride, is used during a life-threatening emergency when the patient exhibits symptoms of cerebral herniation syndrome, any treatment delay can be significant.
Safe Practice Recommendations: To promote safety and allow for the rapid administration of IV hypertonic sodium chloride solutions in emergencies, implement the following risk-reduction strategies:
Procurement and Storage
-
Allow only the pharmacy department to purchase and dispense hypertonic sodium chloride in vials and infusion bags.
-
In the pharmacy, physically separate and store containers of hypertonic sodium chloride in a designated area for IV compounding and admixture supplies.
-
Restrict bags of 3% sodium chloride to the pharmacy and/or certain approved critical care or emergency/urgent care units.
-
When making decisions about stocking hypertonic sodium chloride in patient care units, conduct a robust risk assessment (e.g., failure mode and effects analysis) with an interdisciplinary team (e.g., pharmacists, nurses, physicians). If storage in selected patient care units is allowed, consider the following safeguards:
-
Stock only the 3% sodium chloride bags in patient care units, not the 23.4% sodium chloride vials (do not stock 23.4% sodium chloride vials outside of the pharmacy)
-
For hospitals without 24-hour pharmacy services, stock 23.4% sodium chloride vials, if needed, in a single, secure critical care location that only a few trained professionals (e.g., house/ critical care supervisor, intensivist) can access after pharmacy hours for emergencies
-
-
Stock only in approved critical care or emergency/urgent care units
-
Stock in limited quantities
-
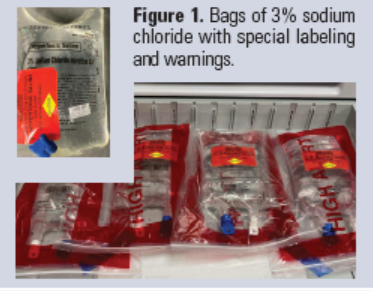
Label with a customized high-alert medication label and bold warnings (Figure 1)
-
Store in a separate locked/lidded compartment, segregated from other medications; avoid storage in matrix drawer configurations
-
If stocked in an ADC, do not allow access via override (override access for a few trained professionals may be necessary but only in facilities without 24-hour pharmacy review of orders)
-
-
To prevent mix-ups with 5% dextrose solutions, do not procure, order, or stock IV containers of 5% sodium chloride anywhere in the facility (even the pharmacy).
Prescribing
-
Create standardized protocols and order sets for each indication of IV hypertonic sodium chloride (e.g., ICP, hyponatremia) that allow for different dosing units as necessary (e.g., ICP: mL/kg [bolus] and mL/kg/hour [infusion]; hyponatremia: mEq/kg [bolus] and mEq/kg/hour [infusion]), and match how the practitioner must program a smart infusion pump, when needed.
-
Update the nomenclature in order entry systems (and ADC screens as applicable) to include “HYPERTONIC” for any sodium chloride product greater than 0.9% concentration. Consider using “HYPERTONIC” for 3% sodium chloride injection and “CONCENTRATED” for 23.4% sodium chloride injection for further differentiation. Never refer to “HYPERTONIC” or “CONCENTRATED” sodium chloride as “saline.”
-
Build alerts in the provider order entry system to warn staff about high serum sodium levels in patients receiving hypertonic sodium chloride, reaching/exceeding maximum or critical doses, and hypertonic sodium chloride orders for patients located outside of a critical care or an emergency/urgent care unit.
-
Require all orders from non-physician prescribers, residents, and fellows for IV hypertonic sodium chloride to be approved by an attending physician or intensivist with proper credentials.
-
Default all hypertonic sodium chloride orders to “stat,” giving them higher priority and moving them to the top of the queue for pharmacy verification to avoid delays.
-
Restrict the prescribing of 23.4% sodium chloride to patients with refractory intracranial hypertension and/or cerebral herniation syndrome.
Dispensing
-
Do not manually compound base solutions requiring concentrations of sodium chloride that are available in commercially premixed solutions (e.g., 0.45%, 0.9%, 3%); instead use the commercially available premixed solutions.
-
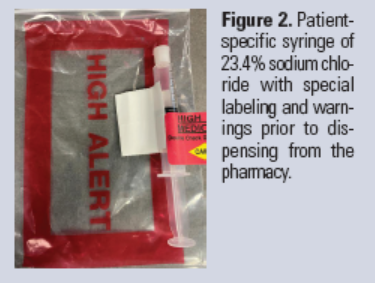
When possible, prepare and dispense IV push doses of 23.4% sodium chloride used in critical care or emergency/urgent care units from the pharmacy, labeled with appropriate warnings (Figure 2), and hand-deliver the patient-specific dose to the healthcare professional administering the drug.
-
Require barcode scanning and an independent double check before dispensing hypertonic sodium chloride to a patient care unit, both for stock and patient-specific use.
Administration
-
In indication-based protocols for IV hypertonic sodium chloride, include directions for administration (e.g., rate of administration, the concentration at which administration through a central IV access line is required) and the type and frequency of patient monitoring required during administration.
-
If hypertonic sodium chloride is available in an ADC, do not allow staff to access it via override. Require verification by a pharmacist prior to removing the drug within the patient’s profile for administration (see bullet under Procurement and Storage if facilities do not have 24-hour pharmacy services).
-
Build a clinical advisory or alert in the smart infusion pump to enter the dose appropriately (e.g., mL, mEq) based on the indication or use.
-
Provide pump programming guidance in the protocols or on the patient’s medication administration record.
-
Require barcode scanning of the patient for identification and of the product as well as an independent double check of the product, concentration, dose, patient, pump programming, and access line prior to administering IV hypertonic sodium chloride.
-
Consider building a smart infusion pump drug library entry with maximum dose limits and using a syringe pump to deliver doses of 23.4% sodium chloride.
-
Allow only trained, licensed, independent practitioners and registered nurses in critical care units and the emergency department to administer IV hypertonic sodium chloride. Consider requiring the attending physician or an intensivist to be at the bedside during administration.
-
Administer hypertonic sodium chloride via a central line if possible (23.4% sodium chloride must be administered via a central line).
Monitoring
-
For patients receiving hypertonic sodium chloride, monitor serum sodium levels at baseline and at least every 6 hours, as well as renal function studies as needed for signs of acute kidney injury and unwanted acidosis.
-
Monitor the patient for possible side effects of hypertonic sodium chloride (e.g., rebound elevated ICP, renal impairment, subarachnoid hemorrhage, natriuresis, high urinary water losses, hyperchloremic acidosis, masking of diabetes insipidus1,6).
References
- Kochanek PM, Tasker RC, Carney N, et al. Guidelines for the management of pediatric severe traumatic brain injury, third edition: update of the Brain Trauma Foundation guidelines. Pediatr Crit Care Med. 2019;20(3S Suppl 1):S1-S82.
- Weed LH, McKibben PS. Pressure changes in the cerebro-spinal fluid following intravenous injection of solutions of various concentrations. Am J Physiol. 1919;48(4):512-30.
- Cook AM, Jones GM, Hawryluk GWJ, et al. Guidelines for the acute treatment of cerebral edema in neurocritical care patients. Neurocrit Care. 2020;32(3):647-66.
- James HE, Langfitt TW, Kumar VS, Ghostine SY. Treatment of intracranial hypertension. Analysis of 105 consecutive, continuous recordings of intracranial pressure. Acta Neurochir (Wien). 1977;36(3-4):189-200.
- Fisher B, Thomas D, Peterson B. Hypertonic saline lowers raised intracranial pressure in children after head trauma. J Neurosurg Anesthesiol. 1992;4(1):4-10.
- Qureshi AI, Suarez JI. Use of hypertonic saline solutions in treatment of cerebral edema and intracranial hypertension. Crit Care Med. 2000; 28(9):3301-13.
Access this Free Resource
You must be logged in to view and download this document.