
Lack of Standard Dosing Methods Contributes to IV Errors
Problem: As the use of parenteral medications increases, improvements in drug infusion technology have enhanced our ability to dose these medications very precisely. However, a variety of dosing methods, such as mcg/kg, mcg/kg/minute, mcg/kg/hour, and many others exist, and few drug-specific dosing norms have been established. It is common to find multiple dosing methods used for a single drug (see Table 1).1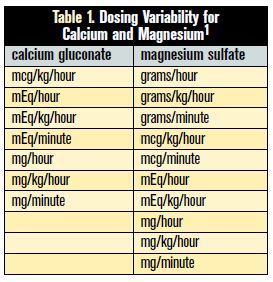 Unfortunately, the lack of standardization makes selection of the proper dosing method difficult, and errors are common. Some mix-ups have involved using the wrong dosing method when prescribing medications. For example, Lesar found that the dosing method was wrong in 29.5% of 200 consecutive prescribing errors with potentially adverse outcomes, particularly with pediatric patients.2 Other errors have involved the misprogramming of pumps when selecting the dose, dosing method, or infusion rate. A recent example of an error reported this month follows.
Unfortunately, the lack of standardization makes selection of the proper dosing method difficult, and errors are common. Some mix-ups have involved using the wrong dosing method when prescribing medications. For example, Lesar found that the dosing method was wrong in 29.5% of 200 consecutive prescribing errors with potentially adverse outcomes, particularly with pediatric patients.2 Other errors have involved the misprogramming of pumps when selecting the dose, dosing method, or infusion rate. A recent example of an error reported this month follows.
An 80-year-old comatose man (80 kg) from a long-term care facility was taken to an urgent care center for treatment of urosepsis and septic shock. Among other intravenous fluids and medications, dopamine (400 mg/500 mL) was ordered in a mcg/kg/minute dose to treat persistent hypotension, with increasing titration prescribed to maintain his blood pressure. Over the next hour, the infusion was titrated upward two more times in 5 mcg/kg increments with no response. A critical care transport service was called to transport the patient to a nearby hospital for admission to a critical care unit.
When the transport team arrived, one of the paramedics reviewed the patient’s IV infusions and, per protocol, independently calculated the rate of infusion for each. While reviewing the pump settings, the paramedic noticed that the dopamine dose had been programmed in mcg/kg/HOUR, not mcg/kg/MINUTE. Although a Baxter Colleague smart pump had been used to program the initial infusion, the nurse had elected to bypass the pump library and instead used the pump in the dose calculator mode. On the screen to choose dosing options, the nurse accidentally selected mcg/kg/hour, which appeared on an alphabetical list before mcg/kg/minute, a potential error-promoting pump feature since mcg/kg/minute is used more frequently than mcg/kg/hour. After the pump was reprogrammed to deliver the correct dose, the patient’s blood pressure increased and he became conscious. The patient was subsequently transported to the nearby hospital and discharged 5 days later.
When reporting this error to the receiving hospital where the patient had been transported, the paramedic learned that the same type of error had been reported previously in the past 6 months. In fact, ISMP has received many reports regarding selection of the wrong dosing method when programming pumps. To cite another recent example—this one from the Pennsylvania Patient Safety Reporting System—an order for propofol 80 mcg/kg/ HOUR for an elderly man was administered at 80 mcg/kg/MINUTE due to a pump programming error, resulting in oversedation but no additional harm. A similar type of error involves mix-ups between mcg doses and mcg/kg doses. In one case, a 3 kg infant received a 36 mcg bolus dose (12 mcg/kg) of fentanyl instead of a 12 mcg dose (4 mcg/kg). Using a Smiths Medical Medfusion 3500 Syringe Pump with smart pump technology, the nurse did not notice that the pump had prompted for a mcg/kg dose, not a total dose. She subsequently entered “12” into the pump, which calculated a dose of 36 mcg (12 mcg/kg) for the 3 kg infant. In this case, a soft dose-limit alert had displayed on the pump, and another nurse had double-checked the pump settings, but the alert was overridden, and the drug was administered. Later that day, the infant received a 1.8 mg bolus dose of midazolam instead of the intended dose of 0.6 mg after the same programming error was made.
The wide variability of dosing methods seen in practice settings contributes to the risk of pump programming errors. Two years ago, a review of smart pump drug library sets from more than 100 independent hospitals revealed just how large a problem this is: Table 1 illustrates an extensive range of dosing options for familiar medications such as calcium gluconate and magnesium sulfate.1 Variability was also revealed within hospitals—sometimes within a single unit—for the same drug (excluding differences explained by adult and pediatric dosing).
Safe Practice Recommendations
Healthcare organizations should consider the following suggestions to reduce the risk of IV dosing errors:
Standardize dosing methods. Look for variable dosing methods for the same medication in your hospital, and select a standard way to dose the drug for adults and a standard way to dose the drug for pediatric patients. Also examine the different dosing methods used in the organization for all drugs, and to the extent possible, standardize the dosing methods to promote familiarity. Health systems comprising multiple hospitals will also benefit from system-level standardization, as patients and nurses may transfer among the facilities. List the standard dosing methods on preprinted or electronic order sets in which applicable drugs appear.
Use fully functional smart pumps. Use of smart pumps that provide dosage error-reduction software will help avoid harmful mix-ups among various dosing methods for the drugs in the pump’s library. Other safety features include unchangeable dosing units once a drug is selected, weight limits, and clinical advisories. Smart pump alerts warn practitioners of impending medication errors and should not be overridden. If an alert is activated, it is crucial for the practitioner to investigate the warning and act accordingly. Organizations should conduct regular compliance rounds to ensure that the dose-checking capabilities are fully functional, as well as review available data from the error-reduction software to monitor appropriate staff interaction with the technology.
List dosing methods on MARs and labels. When possible, the dose of a medication should be displayed on the medication administration record (MAR) and the drug container label the same way the information will be needed to program the pump.
List dosing methods on orders. Prescribers should list the dosing method used along with the calculated dose of drugs at risk for error (e.g., pediatric drugs, chemotherapy).
Verify the dosing method. When applicable, pharmacists and nurses should verify both the dosing method used and the calculated dose before dispensing or administering a medication.
Verify pump settings during hand-offs. Verify all pump settings upon transfer of patients and at the beginning of each shift. Be sure the dosing method and total dose make sense for the patient given his or her weight, age, and condition.
Suspect an error. If a patient is not exhibiting the physiologic changes that would be expected given the infusion, consider the possibility of an error, and verify the pump settings.
Use simulation training. To heighten staff awareness about mix-ups with dosing methods, consider simulation training in which participants investigate a hypothetical case with a dosing error, uncover the error, and take corrective action.
References: 1) Bates DW, Vanderveen T, Seger DL, et al. Variability in intravenous medication practices: implications for medication safety. Jt Comm J Qual Pat Saf 2005;31:203-10. (Table reprinted with permission.) 2) Lesar TS. Errors in the use of medication dosage equations. Arch Pediatr Adolesc Med 1998;152:340-44.