
ISMP Survey Provides Insights into Preparation and Admixture Practices OUTSIDE the Pharmacy
In our August 2020 ISMP Nurse AdviseERR newsletter, we invited practitioners who prepare and/or admix sterile, injectable medications and/or infusions OUTSIDE the pharmacy to participate in a survey. The purpose of the survey was to learn about the frequency of preparing and admixing medications and/or infusions outside the pharmacy; the extent of implementing safe preparation and admixture practices; the training associated with medication preparation and admixture; the occurrence of preparation and admixture errors; and the perceived safety challenges associated with medication and/or infusion preparation and admixture. A description of the survey findings follows.
Respondent Profile
ISMP thanks the 444 practitioners who participated in our survey, providing us with an in-depth look at current sterile, injectable medication and/or infusion preparation and admixture practices outside the pharmacy. Most survey respondents were nurses (77%, including advanced practice nurses) and anesthesia providers (8% certified registered nurse anesthetists and anesthesiologists). The remaining respondents (15%) included decentralized pharmacists or technicians who prepare and admix medications and/or infusions in clinical areas, as well as physicians, supervisors, and others.
Most (81%) survey respondents worked in an acute care or specialty hospital while others worked in an ambulatory surgery center (5%), ambulatory infusion center (3%), physician practice setting or clinic (3%), or long-term care facility (1%). The remaining respondents (7%) described a variety of other work settings such as a critical access hospital, home health organization, emergency medical services provider, freestanding emergency department, infirmary, or outpatient dialysis center. The clinical setting in which respondents worked was also diverse, with most reporting adult medical-surgical (28%), adult critical care (14%), perioperative (13%), and emergency (13%) settings. Seven percent of respondents reported their clinical setting as outpatient; 6% worked in labor and delivery; 5% worked in pediatric settings; and 3% worked in oncology settings. Most (11%) of the remaining respondents reported working in multiple clinical settings or a highly specialized clinical setting (e.g., cardiac catheterization, interventional radiology, hyperbaric chamber, hemodialysis).
Type and Frequency of Preparation and Admixture
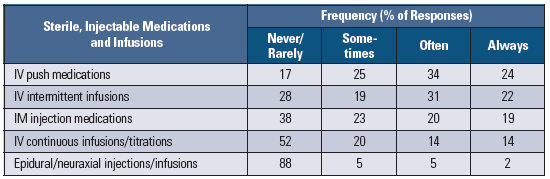
Respondents reported that the types of sterile injectables most frequently prepared outside the pharmacy (Table 1) were:
-
Intravenous (IV) push medications, mostly medications transferred from vials to syringes (e.g., opioids, antiemetics, antibiotics, proton pump inhibitors)
-
IV intermittent infusions, mostly minibag diluent containers with integral vial adaptors (e.g., MINI-BAG Plus)
-
Intramuscular (IM) injections, mostly vaccines, antipsychotics, and antibiotics (e.g., cefTRIAXone)
More than a quarter (28%) of respondents also reported often or always admixing IV continuous infusions or titrations, particularly insulin, vasopressors, or lifesaving drug infusions required during emergencies. An additional 20% of respondents reported sometimes admixing IV continuous infusions or titrations. Most (88%) respondents reported rarely or never preparing or admixing epidural/neuraxial injections or infusions outside the pharmacy. Respondents who reported always or often preparing or admixing epidural/neuraxial injections or infusions (7%, n = 32) were mostly anesthesia providers, advanced practice nurses, and pharmacists, although more than one-quarter (n = 9) of those respondents were nurses.
Table 1. Frequency of preparing/admixing sterile, injectable medications/infusions outside the pharmacy
Preparation and Admixture Practices and Training
When respondents were asked about their agreement or disagreement with five best practices associated with preparing or admixing sterile, injectable medications and/or infusions outside the pharmacy (Table 2), preparing or admixing one medication/infusion at a time generated the highest level of agreement, with 84% of respondents agreeing or strongly agreeing. Establishing standard processes for preparation, admixture, and labeling generated moderate agreement; however, fewer respondents strongly agree that these procedures are being followed. More than half (53%) of all respondents disagree or strongly disagree that their organization requires practitioners who prepare or admix sterile, injectable medications and/or infusions to undergo formal training. Similarly, almost half (49%) of respondents disagree or strongly disagree that they have been formally trained for this important and complex task.
Table 2. Percent of agreement or disagreement with best practices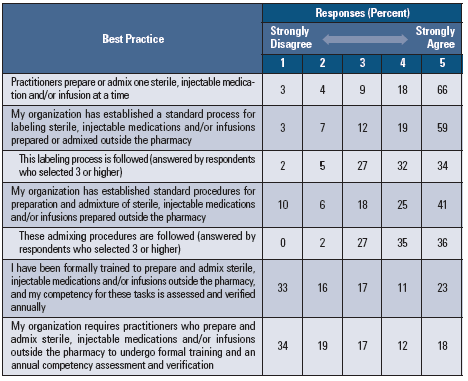
Half (50%) of respondents reported learning how to perform sterile, injectable medication and/or infusion preparation and admixture tasks during their professional training or residency program. Only 16% of respondents said they had received “on the job” training during orientation; however, 32% reported no formal training or annual competencies at all for these tasks.
Selecting among all applicable choices, most respondents reported preparing and admixing medications and/or infusions in an area dedicated for this purpose, such as a medication room (71%), segregated area designated for mixing sterile ingredients (25%), anesthesia workstation (18%), or in a laminar airflow hood located outside the pharmacy (4%). However, less ideal locations for preparation and admixture were also reported, including at the bedside (37%), on a counter or desk in the nursing station (28%), and on a computer workstation (16%). Eight percent of respondents reported preparing and/or admixing medications in the operating/procedure room, patient’s home, ambulance, or elsewhere.
Only 35% of respondents are required to have another practitioner independently double check that certain medications or infusions have been prepared properly outside the pharmacy prior to administration. Among these respondents, 30% reported that all high-alert medications require an independent double check, while another 44% indicated that only certain high-alert medications (e.g., vasoactive agents, oxytocin, insulin, opioids, thrombolytics) require such checks. However, it is likely the types of medications or infusions requiring an independent double check is dependent upon the types of medications prepared or admixed outside of the pharmacy in any given organization. Furthermore, it was not clear from the survey results whether independent double checks for admixtures occurred before a medication was added to a diluent, as it should be required in a pharmacy, or much later at the bedside.
Preparation and Admixture Errors
Almost one-third (31%) of respondents were aware of or personally experienced errors when preparing or admixing sterile, injectable medications and/or infusions during the past 12 months. Among all respondents, 69% were unaware or uncertain whether an error had occurred. Since the practitioner preparing the medication or solution is often the one administering it, the detection of an error is less likely, especially given the low rate of independent double checks noted by respondents. Most respondents who reported awareness of an error reported various types of errors, including:
-
Use of an expired drug (or not administering the medication/infusion immediately after preparation) (90%)
-
Use of the wrong drug, dose, concentration, diluent, or diluent volume (82%)
-
No label or labeling error (81%)
-
Wrong preparation technique (e.g., improper use of multiple-dose vials, not using a filter needle) (80%)
Numerous respondents also mentioned the failure to activate minibags with integral vial adaptors as an error type, leading to the administration of just the diluent without the drug.
The most common errors that were personally experienced included wrong preparation technique (21%); incorrect diluent/diluent volume (20%); incorrect dose/concentration/volume (19%); and no label/labeling error (19%).
Biggest Safety Challenges
ISMP received comments from 281 survey respondents when asked about the biggest safety challenge they face related to preparation and admixture of sterile, injectable medications and/or infusions outside of the pharmacy. We have aggregated almost all of the comments into various categories and presented the most common in Table 3. While the reported challenges were diverse, the most frequently cited challenge was rushing through the preparation or admixture process, especially during emergencies requiring lifesaving, high-alert medications. Many respondents reported feeling ill-prepared to follow processes designed for routine situations under critical, time-sensitive conditions. Numerous respondents noted that, when rushed, the admixture process was often completed by memory, without time to reference standard procedures. Many respondents reported they also worry about the sterility of the preparation area, admixture process, and the end product.
Table 3. Biggest safety challenges with the preparation/admixture of sterile, injectable medications/infusions outside of the pharmacy (n = 281 respondents)
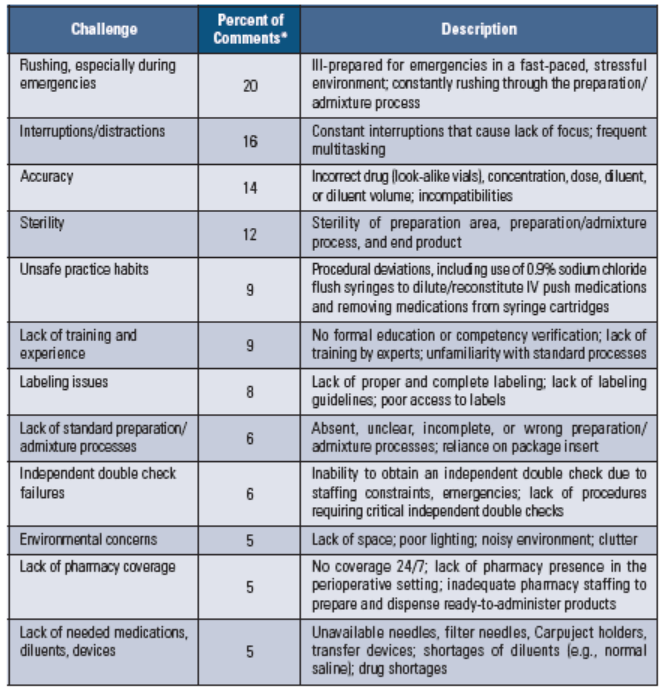
Interruptions, distractions, and concerns about the accuracy of the final product were also frequently mentioned as challenges, especially when more than one vial or a partial vial was needed or when admixing high-concentration infusions. Along with a lack of training and experience, unsafe practices like using flush syringes to dilute or reconstitute IV push medications were also cited as safety challenges. Of note, several respondents commented that they were worried about unfamiliarity with the process when the rare lifesaving task of preparation and admixture is required. Additional challenges were mentioned related to labeling issues; lack of standard preparation and admixture processes; independent double check failures; environmental concerns; lack of pharmacy coverage; and lack of needed medications, diluents, and equipment.
Summary
Although a great deal of emphasis has been placed on the safety and quality of preparing and admixing compounded sterile preparations in the pharmacy, the preparation and admixture of sterile, injectable medications or infusions outside the pharmacy occurs frequently, particularly for IV push medications, IV intermittent infusions, and IM injections. Almost half of the survey respondents admix IV continuous infusions and titrations more than 10% of the time, often involving high-alert medications that can result in serious patient harm if errors occur. Eighty-one percent of respondents report that preparation and admixture occur in less than ideal locations such as the bedside, the counter in a nursing station, or on a computer workstation. Only about one-third of survey respondents reported their institution requires an independent double check of certain sterile, injectable medications and/or infusions that have been prepared or admixed outside of the pharmacy.
Most survey respondents report their organization has established standard processes for preparing, admixing, and labeling of sterile injectables and/or infusions outside of pharmacy; however, they also report lower confidence with staff following these processes, especially during emergencies when human memory is relied upon.
Staff training for preparation and/or admixture of sterile, injectable medications and/or infusions is a significant challenge, with about half of the survey respondents reporting no formal training, which was often not required by their organizations. Almost one-third of respondents reported no formal training or annual competencies at all, and another 16% reported “on the job” training only during orientation, which may have occurred years ago. The lack of formal training was also listed as the biggest challenge by 9% of respondents.
Almost one-third of survey respondents were aware of or personally experienced an error during preparation and/or admixture of injectable medications and/or solutions in the past 12 months. Most of the known errors were associated with the accuracy of the final product, which could result in patient harm.
The biggest safety challenges cited by respondents were rushing through the preparation/ admixture process, especially during emergencies, completing preparation/admixture by memory, interruptions and distractions, and concerns about sterility and accuracy.
Access this Free Resource
You must be logged in to view and download this document.