
ISMP Survey Provides Insights into Pharmacy Sterile Compounding Systems and Practices
Millions of compounded sterile preparations (CSPs) are produced each year, many in hospital pharmacies. In our July 30, 2020 acute care newsletter, we invited pharmacists and pharmacy technicians who prepare or oversee the production of CSPs to participate in a survey on pharmacy compounding. The purpose of the survey was to:
-
Increase awareness of the best practices associated with pharmacy sterile compounding
-
Assist pharmacy staff with identifying opportunities to improve the safety of sterile compounding
-
Learn about the extent of implementing safe pharmacy compounding practices, the use of pharmacy compounding technologies, and the occurrence of pharmacy compounding errors
-
Identify the most significant, perceived safety challenges related to pharmacy sterile compounding
An overview of the survey findings follows.
Respondent Profile
More than 600 (N = 634) pharmacy practitioners participated in our survey. Most respondents were pharmacists (80%) and pharmacy technicians (18%), although a few (2%) were pharmacy students/residents or medication safety officers (MSOs). Respondents were split regarding their position level, with 46% identifying as ‘staff’ and 47% identifying as a ‘manager/director’ or ‘administrator.’ Most of the remaining respondents (7%) listed their position as ‘instructor,’ ‘lead,’ ‘coordinator,’ or ‘supervisor.’ Most respondents work in a hospital pharmacy (87%). The remaining work in an ambulatory infusion center (5%); an outpatient/compounding pharmacy (3%); or in home infusion centers, specialty hospitals, home care, or research (5%). Only 4% of the survey respondents reported that their facility is registered as a 503B compounding pharmacy. In addition to ‘sterile to sterile’ compounding utilizing already manufactured prepared products in vials and bags, 19% of respondents also prepare ‘non-sterile to sterile’ compounded preparations utilizing active pharmaceutical ingredients as the starting material. ‘Non-sterile to sterile’ compounding accounts for approximately 10% (range of less than 1% to 30%) of all CSPs in these facilities.
Compounding Technologies
More than half of all respondents (57%, n = 361) reported using technologies when compounding sterile preparations, which include:
-
Barcode verification systems without images (48% use this technology for approximately 75% [range of 10-100%] of all CSPs)
-
Workflow systems that use barcode verification and images (47% use this technology for approximately 75% [range of 5-100%] of all CSPs)
-
Automated multiple ingredient compounding devices (e.g., parenteral nutrition [PN] compounders) (46% use this technology for approximately 10% [range of 1-100%] of all CSPs)
-
Image sharing or remote video supervision of the sterile compounding process (32% use this technology for approximately 50% [range of 5-100%] of all CSPs)
-
Pharmacy workflow systems with images and barcode scanning and/or gravimetric verification (25% use this technology for approximately 50% [range of 1-100%] of all CSPs, mostly for antineoplastics and PN)
-
Intravenous (IV) sterile compounding robot (8% use this technology for approximately 30% [range of 5-100%] of all CSPs, mostly for antineoplastics and PN)
Sixty-three percent of respondents who utilize images to verify CSPs stop production for verification of certain drugs, diluents, and doses before mixing the ingredients and completing the compounding process. In some cases, all medications require verification before mixing; however, for most of these respondents, only certain medications require verification prior to mixing, including the following:
-
All or certain hazardous drugs (e.g., antineoplastics)
-
All or certain high-alert medications (e.g., insulin, opioids/other controlled substances, epidural/intrathecal medications, epoprostenol)
-
All or certain blood products (e.g., KCENTRA [prothrombin complex concentrate, [human])
-
All pediatric and/or neonatal medications
-
Biologics including monoclonal antibodies
-
Medications requiring dilution
Safe Compounding Practices
ISMP identified nine best practices associated with pharmacy sterile compounding and asked survey respondents to evaluate their degree of implementing these best practices (Table 1). Respondents reported the highest level of implementation (73% always, 15% often) with ensuring that there are enough workbenches in the cleanroom/sterile compounding area to support only one staff member working at a time per primary engineering control device (e.g., laminar airflow workbench, biological safety cabinet, isolator). For respondents who reported lower compliance with this best practice, comments suggest that the degree of implementation is dependent on the pharmacy’s location (central vs. satellite), time of day, urgency of preparing the CSP, and overall workload.
Table 1. Implementation of compounding best practices (in descending order based on overall level of implementation)
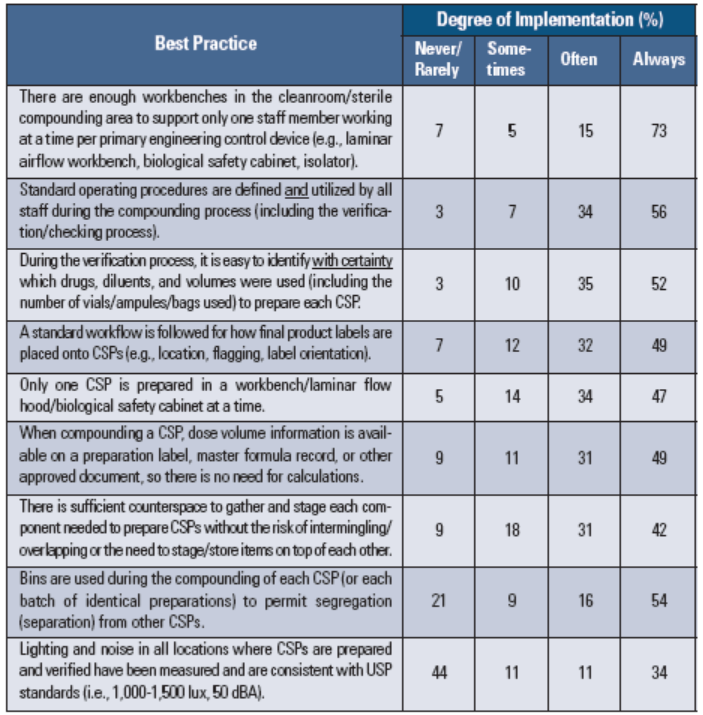
More than half of all respondents (56%) reported that standard operating procedures are defined and always followed during the compounding process (including the verification/checking process). Another one-third (34%) of respondents reported that the procedures are defined and often followed. However, pharmacy technicians tended to report higher compliance with always following compounding procedures than what was perceived by pharmacists (62% vs. 54%, respectively). Ten percent of respondents reported that standard procedures are never, rarely, or sometimes defined and followed. Comments suggest that the procedures might be well defined but that shortcuts may be taken to improve efficiency and production numbers. Numerous examples of at-risk procedural violations were provided (e.g., hand hygiene, jewelry, makeup, nail protocols not followed; verification process from the doorway). A few comments suggested that pharmacists and technicians utilize their own process rather than following standard procedures.
Alarmingly, only 52% of respondents reported that it is always easy to identify with certainty which drugs, diluents, and volumes were used (including the number of vials/ampules/bags used) when verifying the preparation of each CSP. However, again, pharmacy technicians tended to report higher confidence with always being able to identify which drugs, diluents, and volumes were used to prepare each CSP than was perceived by pharmacists (62% vs. 48%, respectively). Respondents with high confidence in identifying drugs, diluents, and volumes during verification indicated that cameras, image capture, verification software, and/or pharmacy workflow systems were used. However, many respondents commented on technology limitations (e.g., picture quality) or shortcuts (e.g., bypassing technology) that raised concerns. Respondents with the lowest confidence in the verification process tended to cite weaknesses in the outdated and error-prone post-production syringe pull-back method of verification. Numerous respondents commented that diluents were not easy to identify, particularly if they had been withdrawn from bulk stock bags or bottles that stayed in the hood and for which a syringe drawn back to the diluent volume was not even included for verification. Others noted that vials and syringes sometimes get mixed up if there is a large array of CSPs on a cart to verify.
Almost half of all respondents (49%) reported that they always follow a standard workflow for how final product labels are placed onto CSPs. Pharmacy technicians tended to report higher compliance with always following a standard process for label placement on CSPs than perceived by pharmacists (58% vs. 46%, respectively). Almost one in five respondents (19%) reported wide variation in label placement, and most of the survey comments noted that there is no standard process in place.
Slightly less than half of all respondents (47%, always) also reported that only one CSP is prepared at a time. Respondents’ comments noted exceptions for products that take a long time to dissolve or reconstitute (20-30 minutes), stating that these products are put aside while preparing another CSP. A few respondents commented that they also keep partially used vials of medications and bags of diluents in the hood.
Nearly half of all respondents (49%) reported that dose volume information is always available on a preparation label, master formula record, or other approved document, so there is no need for calculations. However, again, technicians tended to report higher full compliance than perceived by pharmacists (58% vs. 46%, respectively). One in five respondents (20%) reported that this best practice is followed half of the time or less. Most comments suggested that prep labels are not ideal, and calculations may be necessary to determine the volume of ingredients if the label only expresses the dose in mg (or g, units, etc.). A few respondents reported that the total volume is not always provided on labels. Quite a few respondents noted that they double check all calculations on prep labels, noting specific label errors in some cases.
Best practices associated with sufficient counterspace to gather and stage each CSP, the use of bins to permit separation of CSPs, and measurement of lighting and noise to ensure consistency with USP standards scored lowest in our survey based on overall level of implementation. Comments from respondents laid bare their pervasive concerns about pharmacy space limitations, inconsistent use of bins to separate each CSP, and the lack of knowledge around measurement and standards related to noise and lighting levels in the pharmacy.
Sterile Compounding Errors
Nearly three-quarters (74%) of all survey respondents were aware of at least one pharmacy sterile compounding error that had occurred during the past 12 months, including those caught and corrected in the pharmacy as well as those discovered after dispensing. A higher percentage of pharmacists (79%) were aware of these errors than technicians (67%). The types of reported pharmacy compounding errors included:
-
Incorrect dose or concentration (58%)
-
Incorrect base solution (51%)
-
Incorrect base solution volume (43%)
-
Issue or error (including omission) with labeling of a CSP (41%)
-
Incorrect reconstitution of a drug (volume or diluent) (36%)
-
Incorrect drug (35%)
-
Wrong preparation technique (e.g., improper filtering, wrong tubing) (26%)
-
Expired drug, base solution, or CSP (16%)
-
Wrong timing (e.g., preparing an antineoplastic on the wrong date) (12%)
-
Omission of a drug (5%)
Examples of other error types reported (7%) include coring of vials on robots, using the wrong port or container, and wrong patient errors. Only 4% of respondents reported awareness of errors associated with CSPs purchased from 503B compounding pharmacies.
Biggest Safety Challenges
ISMP received more than 600 comments from survey respondents when asked about the biggest challenge they face related to pharmacy sterile compounding. We have aggregated most of the comments into various categories and presented the most common in Table 2. While the reported challenges are diverse and unique to each individual respondent, the most commonly cited challenge was the inability for a pharmacist to accurately verify prepared CSPs if using an indirect process such as the post-procedure syringe pull-back method. The second most common challenge was associated with meeting USP <797> (Pharmaceutical Compounding – Sterile Preparations) and USP <800> (Hazardous Drugs – Handling in Healthcare Settings) standards. The ability to properly train both technicians and pharmacists to prepare and/or verify CSPs was listed as the third biggest challenge, followed by the lack of purchasing and utilizing various sterile compounding technologies, such as cameras, workflow systems, gravimetrics, and bar-coding technology. Additional environmental, human resource, technology, human factors, process, procurement, and leadership issues were described as other pharmacy sterile compounding challenges, as noted in Table 2.
Table 2. Examples of biggest safety challenges related to pharmacy sterile compounding (n = 505)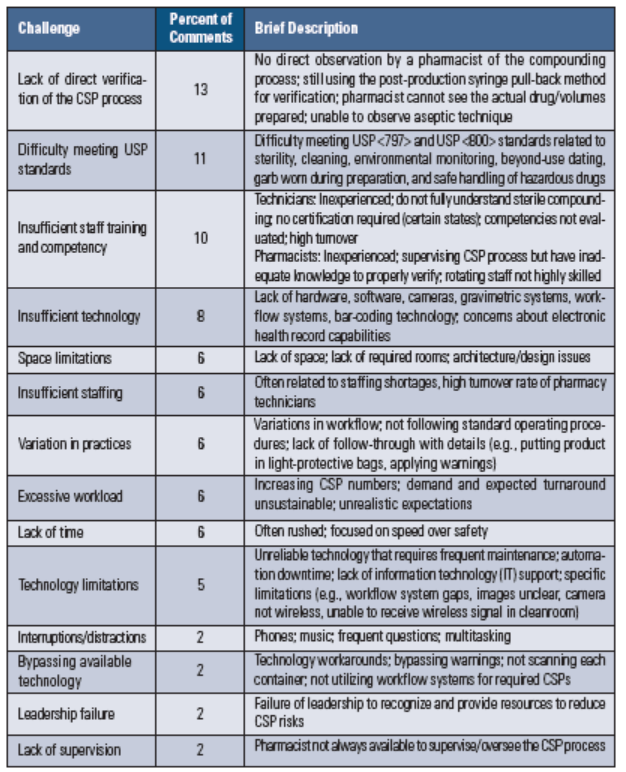
Conclusion
ISMP wants to sincerely thank each and every person who participated in our survey. Your responses provided an in-depth look at current pharmacy sterile compounding practices, which substantially contributed to our shared learning. We plan to utilize and share more detailed survey findings in the future to drive improvements in sterile compounding.
We hope that pharmacies will use the results of this survey to prompt internal discussions about improvements that may be needed in their sterile compounding practices to reduce the risk of errors. If your pharmacy did not participate in this survey, you may want to download it, distribute it internally, and take the survey to pinpoint your vulnerabilities and to establish a plan for improvement. You can also utilize the ISMP Guidelines for Safe Preparation of Compounded Sterile Preparations to guide your discussion and to identify practical ways to improve your CSP preparation process.
Access this Free Resource
You must be logged in to view and download this document.