
Independent Double Checks: Undervalued and Misused: Selective Use of This Strategy Can Play an Important Role in Medication Safety
A manual independent double check of high-alert medications is a strategy that has been widely promoted in healthcare to help detect potentially harmful errors before they reach patients.1-3 However, independent double checks used as a risk-reduction strategy have long been disputed as well as misused in healthcare. Its use has been a source of stress for busy prescribers, pharmacists, and nurses who are short on time. Its impact on safety has been questioned by those who rarely find mistakes during the checking process. Its inconsistent use and variability in how the task is carried out has rendered it incapable of detecting many errors. Its overuse as a risk-reduction strategy for high-alert medications has been called to task given its status as a weak error-reduction strategy, particularly if it is the only safeguard in place. Its frequent misuse as a quick fix for an ailing medication use system has been the bane of managers who have investigated serious errors that have reached a patient due to a failed double-check process.
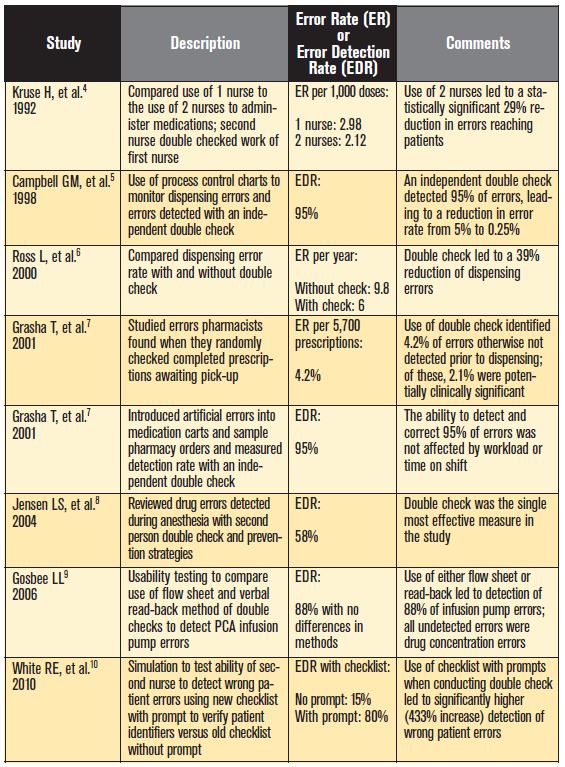
Despite these challenges, ISMP believes that the selective and proper use of independent double checks can play an important role in medication safety. As documented in Table 1, numerous studies have demonstrated the ability of independent double checks to detect up to 95% of errors.4-10 Based on this, an error rate of 5% (1 in 20) can be reduced to 0.25% (1 in 400) by introducing an independent double-check process. While automated double checks such as barcode scanning may yield even better results, there is enough evidence today to suggest that carrying out a manual independent double check is worth the time and effort if this strategy is planned and carried out as follows.
Conduct double checks independently
First, to be most effective, the double check must be conducted independently by a second person5,7-10 to reduce the risk of bias that occurs when the person preparing and checking the medication is likely to see what they expect to see, even if an error has occurred. An independent double check requires two people to separately check each component of the work process. For example, a pharmacist calculates a dose, prepares a syringe of medication, and compares the product to the order; then, a nurse independently checks the order, calculates the dose, and compares the results with the dispensed product for verification. Two people are unlikely to make the same mistake if they work independently. If they work together or influence the checking process by suggesting what the checker should find, both could follow the same path to an error. So holding up a syringe and a vial and saying, “This is 5 units of insulin, can you check it?” is not effective. The person asking for the double check must not influence the individual checking the product in any way.
In the absence of an independent double check, Grasha et al.7 found that delayed self-verification of work conducted hours or days after initial completion has detected errors at rates comparable to those reported with independent double checks; however, Grasha’s work clearly showed that healthcare professionals are better at detecting the errors of others than their own errors. Grasha concludes that double checks work best when they are performed independently.
Use double checks judiciously
With workload issues looming heavily over practitioners, independent double checks should only be used for very selective high-risk tasks or high-alert medications (not all) that most warrant their use. Selected tasks and medications should not be based simply on those which have historically always been double checked, but on a careful assessment of scenarios with the greatest risk. As such, ISMP does not recommend use of an independent check for all high-alert medications or all high-risk tasks. Lack of time to carry out the checking process properly was a strong, recurring theme in studies of failed double checks and staff resistance to this strategy.10,11 Studies of nurses suggest that it may add up to 20 minutes to each medication round to carry out an independent double check for most medications.12,13 Fewer double checks strategically placed at the most vulnerable points of the medication use process will be much more effective than an overabundance of double checks.
Also, do not use double checks as a means of fixing problems when more fundamental system redesign is needed.14 Independent double checks are a poor substitute for system improvements that will actually help prevent errors. Strategies with higher leverage—use of barriers, improving access to information, standardization, and automation, for example—should be considered. Any errors uncovered during the double-check process should also be used for learning and system improvement.
Avoid sole reliance on double checks
Double checks will sometimes fail for a variety of reasons, not the least of which is that the process essentially depends on one fallible person assessing another fallible person’s work. Human performance limits foretell inevitable slips, lapses, and mistakes that will result in an occasional failed check system. The origin of the error can also predict a certain amount of failure with even the most robust independent double-checking process.
An endogenous error arises solely within an individual from a random and unpredictable cognitive event like miscalculating a dose.15 Another person performing the same function will rarely make the same exact mistake. Therefore, endogenous errors are likely to be detected if a double check is performed independently by another person. An exogenous error arises from conditions in the external environment, such as poor design of drug packages and labels, complex task characteristics, or unclear presentation of information.15 Double checks are often less successful in detecting exogenous errors, even when the check is performed independently. Some of the same external factors that initially led to the error are often still present, and people in the same environment could easily make the same mistake during the double check.
Because double-check systems will sometimes fail, the intended improvement in system reliability will be illusory if you rely on these alone to catch all errors. Independent double checks should be bundled with other risk-reduction strategies, and system changes must also be made to reduce the frequency of errors.
Conduct a cognitive review of the medication
Analysis of failed double-check processes and interviews with staff suggest that double checking often becomes a superficial routine task, and people may lose sight of its importance. These failed checking processes can often be traced to common themes: auto-processing in which the person checking the work of another does so in a habitual manner with little real appraisal; a deference to authority in which the person checking the work of someone who outranks them may not ask questions; a reduction of responsibility or overreliance on double checking in which staff believe someone else will catch any mistakes; social interactions that can lead to unrelated conversations that interfere with the checking process; and lack of time.11
What is often missing in the double-check process is a “sterile cockpit” environment without extraneous conversation and a more cognitive review of all components of the medication, beyond verification of the “5 rights,” that require purposeful thought. Is the drug appropriate for the patient? Does the drug’s indication match the patient’s diagnoses or conditions? Is the dose appropriate for this patient? Is the route of administration proper? These questions and more need to be answered independently by the initial clinician preparing the selected medication for dispensing and administration and the second clinician double checking the medication. See Table 2 for other items to consider when conducting an independent double check. Without a cognitive review of the prescribed medication during a double-check process, errors—particularly prescribing errors that may be overlooked if simply matching the drug order with the product—may not be detected and corrected before reaching the patient. 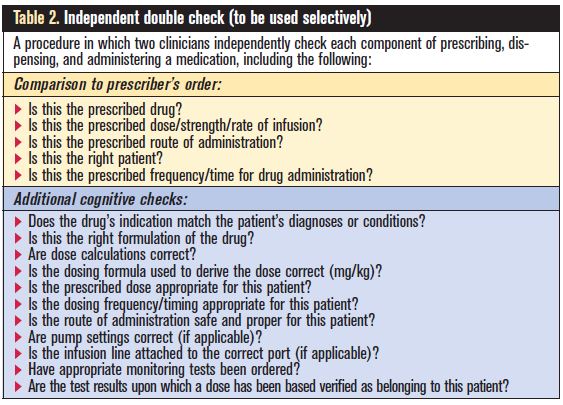
Standardize the process and provide tools
To reduce process inconsistencies, establish a standard process for carrying out an independent double check, and educate staff about its importance and how to carry it out properly—as an independent cognitive task and not a superficial routine task. Make it easy for practitioners to follow the independent double-check process without relying on vigilance and memory.16 For example, add a checklist as a reminder of the components of the process or medication that should be checked and when it should be checked. The questions in Table 2 can be used as a broad template to start an intuitive checklist. However, checklists that include very specific items associated with critical information, rather than more general topics, significantly improve their effectiveness.10 For example, a checklist that instructs users to check the medication label against the original order is not as effective as a checklist that specifies the exact elements to check on the label and the drug order.10 However, design the checklist with care so that the detail does not replace the need for the practitioner to think critically about each aspect of the double-check process. As appropriate, redesign order forms to facilitate crosschecking of information, and make sure the sequence of information on checklists uses the same terminology and follows the logical progression of typical workflow.
Conclusion
In most organizations, a review of the most recent medication errors will likely uncover some aspect of an ineffective double-check process. Take the time to evaluate the procedures for which you require a double check, monitor compliance, assess how often the checks are conducted as designed, and then make the necessary revisions to promote effectiveness. When employed judiciously, conducted properly, and bundled with other strategies, manual independent double checks can be part of a valuable defense to prevent potentially harmful errors from reaching patients.
References
- ISMP. Santa checks his list twice. Shouldn’t we? ISMP Medication Safety Alert! 2009;14(25):1-2.
- ISMP. The virtues of independent double checks—they really area worth your time! ISMP Medication Safety Alert! 2003;8(5):1.
- ISMP. Conducting an independent double-check. ISMP Nurse Advise-ERR. 2008;6(12):1.
- Kruse H, Johnson A, O’Connell D, et al. Administering non-restricted medications in hospital: implications and cost of using two nurses. Aust Clin Rev. 1992;12(2):77–83.
- Campbell GM, Facchinetti NJ. Using process control charts to monitor dispensing and checking errors. Am J Health Syst Pharm. 1998;55(9):946-52.
- Ross L, Wallace J, Paton J, et al. Medication errors in a paediatric teaching hospital in the UK: five years operational experience. Arch Dis Child. 2000;83(6):492–7.
- Grasha T, Reilley S, Schell K, et al. Delayed verification errors in community pharmacy: implications for improving accuracy and patient safety. Technical Report Number 112101. Cognitive Systems Performance Lab. 2001.
- Jensen LS, Merry AF, Webster CS, et al. Evidence-based strategies for preventing drug administration errors during anaesthesia. Anaesthesia. 2004;59(5):493–504.
- Gosbee LL. Test report. Exploration of 2 double-check methods. Institute for Safe Medication Practices Canada. June 2006.
- White RE, Trbovich PL, Easty AC, et al. Checking it twice: an evaluation of checklists for detecting medication errors at the bedside using a chemotherapy model. Qual Saf Health Care. 2010;19(6):562–7.
- Armitage G. Double checking medicines: defence against error or contributory factor? J Eval Clin Pract. 2008;14(4):513-9.
- Alsulami Z, Conroy S, Choonara I. Double checking the administration of medicines: what is the evidence? A systematic review. Arch Dis Child. 2012;97(9):833-7
- Jarman H, Jacobs E, Zielinski V. Medication study supports registered nurses’ competence for single checking. Int J Nurs Pract. 2002;8(6):330-5.
- Truax BT. What is the evidence on double checks? Patient Safety Tip of the Week. The Truax Group. October 16, 2012.
- Senders J. Essays on human error in medicine. ISMP-Canada, October 2000.
- ISMP Canada. Lowering the risk of medication errors: independent double checks. ISMP Canada Safety Bulletin. 2005;5(1):1-2