
Hidden Medication Loss When Using a Primary Administration Set for Small-Volume Intermittent Infusions
While covering for a colleague during patient rounds in an adult medical unit, a pharmacist noticed two empty 50 mL minibags of ZOSYN (piperacillin and tazobactam) hanging on a patient’s intravenous (IV) pole, each attached to a primary administration set. Each primary administration set (BD Alaris pump infusion set) holds about 25 mL of residual volume in the tubing. The implication for this 49-year-old patient with pneumonia was that he had only received about half of the total volume contained in each 50 mL bag, and therefore only half of the Zosyn dose with each intermittent infusion. Additionally, while an extended infusion time of 4 hours had been prescribed for each Zosyn dose, each intermittent infusion was completed in about 2 hours since only half of the volume infused while the other half remained in the tubing. Later, in the room of a 57-year-old patient with cellulitis, the pharmacist found an empty 50 mL minibag of clindamycin, again attached to a primary administration set filled with a residual volume in the tubing, meaning that this patient, too, had only received about half of the dose. Such significant underdoses could have a clinical impact on patient outcomes.1
Background
Medications administered via an intermittent IV infusion (e.g., antibiotics, electrolytes) are typically diluted in a small volume of 0.9% sodium chloride or 5% dextrose in water. If the patient has a compatible primary solution already infusing, these intermittent infusions are often administered through a short secondary administration set attached to a Y-site on the primary administration set, thus minimizing medication loss in the residual volume left behind in the tubing. If the primary solution is not compatible with the intermittent solution, or if the primary solution’s rate of infusion cannot be altered (e.g., heparin) to accommodate the intermittent infusion, a carrier fluid (sometimes called a ‘chaser bag’ or ‘flush bag’) may be ordered. A carrier fluid is a small bag (50 to 250 mL) of compatible fluid that is used as a primary infusion to allow administration of the intermittent infusion via a secondary administration set (A in Figure 1). After the intermittent infusion is complete, the carrier fluid is infused (approximately 25 mL) to flush residual drug from the tubing.
However, when the patient has a vascular access device (e.g., saline lock) placed without a continuously infusing compatible primary solution or carrier fluid, unfortunately, intermittent infusions are often administered using a longer primary administration set (via pump or gravity) connected directly to the patient’s vascular access device (B in Figure 1). This may lead to significant underdosing because the residual volume that exists in the length of the primary administration set may not be administered to the patient.1
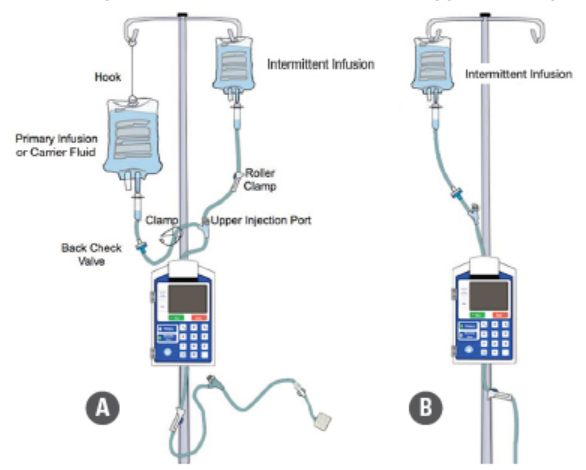
A (left, recommended): Using a secondary administration set attached at the Y-site (upper injection port) of a carrier fluid or primary infusion administration set (minimizes drug loss).
B (right, NOT recommended): Using a primary administration set connected directly to the patient’s vascular access device (leads to significant drug loss).
Nurses may separately flush the tubing of the intermittent infusion to promote administration of the full dose; however, the flush volume would have to be as large as the residual volume left in the primary administration set (e.g., 25 mL). We have also observed the unsafe practice of nurses adding a small volume of extra diluent to small-volume intermittent infusion bags prior to administration to account for the residual volume left in the administration set, risking both errors and contamination. Nevertheless, there would still be medication left in the tubing, which could then be administered to the patient at a later time if the next infusion is administered via the same administration set. Hypothetically, the medication left in the tubing could become contaminated or unstable over time, particularly if it required refrigeration or protection from light prior to administration.1
Scope of the Problem
The pharmacist who observed the small-volume intermittent infusions attached to primary administration sets wondered how often this was occurring. To determine the scope of the problem, he requested monthly reports on the organization’s smart pump technology, including data that showed whether nurses had used primary or secondary administration sets to administer 50 mL infusions. He then determined the number of 50 mL intermittent IV infusions administered to adults correctly as a secondary infusion, excluding chemotherapy (administered via short administration sets). This was divided by the total number of 50 mL intermittent infusions administered as either primary or secondary infusions.
He found that only 28.5% of the 50 mL intermittent infusions had been administered as secondary infusions. The pharmacist then looked at smart pump data from other hospitals within his health system and found that only 35.7% of the 50 mL intermittent infusions had been administered as a secondary solution. Across the entire health system, this represented about 360,000 small-volume (50 mL) intermittent infusions annually that were likely administered to patients at significantly lower doses than prescribed due to using a primary administration set. Based on ISMP’s observations in other organizations and the literature,1,2 the scope of this problem is much larger than only within this health system.
Contributing Factors
To understand why nurses were administering small-volume intermittent infusions via primary administration sets, the pharmacist gathered an interdisciplinary team of nurses, pharmacists, and prescribers, who found the following contributing factors:
Unclear policies/procedures. As with many organizations around the country, the health system found that its organizational and departmental policies and procedures provided few details regarding how to administer small-volume intermittent infusions. A quick search of the literature also found that best practices for administering small-volume intermittent infusions are few; even the Infusion Nurses Society’s Infusion Therapy Standards of Practice document is silent on the issue of whether to administer small-volume intermittent infusions as a primary or secondary infusion.1,3
Lack of awareness. There was a lack of awareness among nurses, pharmacists, and prescribers regarding the significant loss of medication in the tubing when administering intermittent infusions using primary administration sets. Although the risk of medication loss has been widely reported when locating infusion pumps with extension tubing outside patient rooms during the recent pandemic, the issue had not been considered when administering small-volume intermittent infusions using a primary administration set.
Failure to prescribe carrier fluids. When choosing a medication administration method that minimizes the residual volume left behind in the tubing, nurses had limited options if the prescriber ordered an intermittent infusion without a corresponding order for a carrier fluid, or if the prescriber discontinued a compatible continuous infusion while the patient still required intermittent infusions. There were no triggers or reminders for prescribers to order a carrier fluid (and saline flushes), and due to safety and scope-of-practice concerns, nurses were not permitted to hang a carrier fluid without an order.
Recommendations
Results of a recent study suggest that the best practice to minimize medication loss is to administer small-volume intermittent infusions through a secondary administration set with a compatible primary infusion.1 Thus, the pharmacist worked with the interdisciplinary team he had established in his health system and was able to increase the administration of small-volume (50 mL) intermittent infusions as secondary infusions from 35.7% to 77.8% by implementing the following strategies:
Add carrier fluids to order sets. The health system added an appropriate carrier fluid to order sets used for prescribing small-volume intermittent infusions. This contributed to an increase in orders for carrier fluids which enabled nurses to administer intermittent infusions as a secondary infusion and flush the residual volume through the tubing to ensure the patient received the full medication dose. Additionally, pharmacists now have the authority to enter carrier fluid orders without contacting the prescriber. This is particularly important if the patient already has a primary infusion that should continue to be administered at the prescribed rate of infusion. Take, for example, a septic patient who is receiving normal saline at 150 mL per hour. If the patient is also receiving piperacillin/tazobactam in 50 mL over 4 hours three times a day, stopping the saline infusion for 12 hours each day would not be optimal. Instead, a separate compatible carrier fluid, which the pharmacist can now enter, should serve as the primary infusion for the secondary intermittent infusion. At the conclusion of the intermittent infusion, the nurse can then infuse a set amount (approximately 25 mL) of the carrier fluid through the primary tubing.1
Educate staff. The health system increased staff awareness of the significant loss of medication in the residual volume left in the tubing when administering a small-volume intermittent infusion, particularly a 50 mL minibag, as a primary infusion. For nurses, the health system engaged nurse educators, created an educational document on the topic, and came up with a catchy slogan: If the bag is the small kind, put it on a secondary line. They also created a pop-up warning on automated dispensing cabinet screens to administer small-volume intermittent infusions with a secondary set. The pharmacy also affixed labels to minibags stating, “Infuse via secondary set” for the first few months.
Storytelling. The health system also employed a simple but fundamental strategy to create change by conveying compelling stories about errors and the desired change strategy to draw attention to the problem and encourage action. Using actual examples of patients who had likely received only half of the prescribed doses, the stories were shared at departmental and committee meetings, in educational programs, and in “Tip of the Week” documents, which included repetition of the slogan encouraging small bag administration via a secondary administration set.
Lessons Learned
The health system plans to continue working to improve the rate of administering small-volume intermittent infusions as a secondary infusion (improvement has continued at a slower pace since the coronavirus disease 2019 [COVID-19] pandemic). However, they wanted to share with others the lessons they have learned so far:
See the problem firsthand. Do not rely on policies and procedures to illustrate what normally happens when small-volume intermittent infusions are administered. Take the time to observe intermittent infusion administration to understand “real life” practices.
Use data to measure the problem and progress. Historically, practitioner reporting has been used to identify and measure patient safety problems, which provides, at best, an incomplete assessment of whether a problem exists and whether changes have resulted in improvements. More accurate ways of measuring safety problems—through automated technology and direct observation, for example—should be used to identify the scope of suspected safety problems and to monitor progress to determine if improvement efforts have been successful.
Foster collaboration across professions. The importance of fostering teamwork across the professions should not be underestimated. For example, collaboration between prescribers, pharmacists, and nurses may overcome any reluctance to allow post-infusion flushing with a small amount of a compatible carrier fluid. Collaboration across professions is also critical to resolve questions that might arise. How will the organization manage fluid-restricted patients who receive multiple small-volume intermittent infusions? How can an organization minimize instances when a nurse forgets to unclamp the secondary infusion (since the pump may not alarm if the carrier fluid is infusing)? Would it be feasible to program smart infusion pumps to only allow administration of small-volume intermittent infusions as a secondary infusion (may be a concern with interoperability)?
Tell stories to humanize the problem. Storytelling is a familiar form of communication that resonates with all—the contextual details and the exposed humanity in stories educate us, touch us, and inspire us to take action. Storytelling is an efficient vehicle for helping practitioners to understand, remember, and accept new ideas.
References
- Harding M, Stefka S, Bailey M, Morgan D, Anderson A. Best practice for delivering small-volume intermittent intravenous infusions. J Infus Nurs. 2020;43(1):47-52.
- Cousins D. Patients are being underdosed: we need new guidance on small-volume drug infusions. Clinical Pharmacist. 2018;10(12). doi: 10.1211/CP.2018.20205779.
- Gorski L, Hadaway L, Hagle M, McGoldrick M, Orr M, Doellman D. Infusion therapy standards of practice. J Infus Nurs. 2016;39(suppl 1):S1-S159.
Access this Free Resource
You must be logged in to view and download this document.