
Follow ISMP Guidelines to Safeguard the Design and Use of Automated Dispensing Cabinets (ADCs)
Automated dispensing cabinets (ADCs) are decentralized medication distribution systems that provide computer-controlled storage, dispensing, and tracking of medications at the point-of-care in patient care units. This technology was introduced in hospitals in the late 1980s. Although adoption of the technology started slowly, as of 2007, more than 80% of hospitals use ADCs to replace manual floor stock systems and/or medication carts that previously held a 24-hour supply of patient-specific medications in individual patient cassettes.1
Benefits of ADCs
ADCs offer a variety of benefits to the organization and user:
- Provides nurses with increased access to medications in patient care areas to facilitate timely administration of medications
- Ensures locked storage of medications on patient care units and electronically tracks use of controlled substances and other drugs
- Tracks the stocking and distribution of medications to improve inventory control
- Supports the clinical review of medication orders by a pharmacist prior to administration if the ADCs are interfaced with the pharmacy computer
- Can be interfaced with other external databases such as the facility’s admission/discharge/transfer system, and billing systems, thereby increasing the efficiency of drug dispensing and billing
- Can be interfaced with barcode technology to automate the restocking process, track dispensing, and if linked with point-of-care bar-coding systems, ensure an electronic match between the prescribed and selected medication.
What the Research Shows
Based on the benefits described above, ADCs have been recommended as a potential mechanism to increase efficiency as well as reduce medication errors. To date, a small body of evidence has been published regarding the impact of this technology on error rates. Several years ago, Oren et al. conducted a meta-analysis which identified just 7 controlled studies linking ADCs with medication error rates or other secondary endpoints.2 In general, after ADC implementation, these studies identified:
- A reduction in dispensing error rates when filling ADCs compared to manual filling of traditional unit-dose cassettes3,4
- A reduction in drug administration errors (mostly wrong time errors) and fewer missing doses5,6
- A reduction in drug administration errors on a cardiovascular surgery unit, but an increase in errors on an intensive care unit7
- An increase in errors (by more than 30%) in six of seven nursing units evaluated.8
With the exception of wrong-time errors, these studies showed mixed results for reducing drug administration errors with ADCs. Similar results were found by a government-funded compilation of evidence related to ADCs.9 However, many of these studies were conducted before important software and hardware enhancements were available, such as interfaces between ADCs and pharmacy computers, and cabinets with individually lidded compartments. While few studies clearly link ADC design and use to the error rates, error-reporting programs have uncovered several factors that can influence the ability of ADCs to reduce medication errors.
Factors That Influence Safety
ADCs cannot improve safety unless cabinet design and use are planned and implemented with attention to the following factors.
Patient profiling. If the ADC is linked to the pharmacy computer, a pharmacist can review each new medication order and screen it for safety before the drug can be removed from the cabinet—a feature that facilitates The Joint Commission’s requirement for such a review. Without this feature, nurses may not be alerted to unsafe doses, potential allergic reactions, duplicate therapy, contraindications, drug interactions, or other important drug information. An example from the ISMP Medication Errors Reporting Program (ISMP MERP) follows.
Before colchicine was removed from the market last year, a patient died after receiving 10 mg of colchicine IV. The physician had prescribed “colchicine 1.0 mg IV now,” but the decimal point was poorly visible. This, and the use of a trailing zero, led the nurse to believe the dose was 10 mg. If a pharmacist had prescreened the order, the nurse would have been instructed to remove one ampul of colchicine (1 mg) to administer the dose. However, the error reached the patient because the ADC was not profiled to the pharmacy computer, and there was an excessive quantity of colchicine in storage: ten 1 mg ampuls. Thus, the nurse was able to remove enough ampuls to administer the fatal dose.
Overrides. Even when ADCs employ patient profiling, this feature is sometimes overridden to allow removal of drugs in an emergency. However, misuse of overrides has resulted in errors, as in the following example from the Pennsylvania Patient Safety Reporting System (PA-PSRS).
A physician prescribed ZOSYN (piperacillin and tazobactam) for a patient. The first dose was given in the emergency department, and a second dose was given on the medical unit. Both doses were retrieved from an ADC prior to review by the pharmacy. However, when pharmacy reviewed the order, it was noted that the patient had a documented allergy to penicillin. Luckily, the patient did not experience a serious allergic reaction.10
Overrides are not the only examples of workarounds used to access medications from ADCs. Other types of workarounds include use of the “inventory” function (designed to determine the current number of doses of a particular medication on hand) to gain access to medications for patients before pharmacy screening, removing a larger quantity of medications than ordered for one patient, and removing medications for multiple patients while the cabinet is open.
Number and placement of devices. If a sufficient number of ADCs is not available on the unit, nurses may remove doses ahead of time due to limited access during busy drug administration times. Placement of the devices in areas with high traffic or low illumination can also lead to distractions and misread screens or labels.
Screen set-up. Choosing the wrong medication from an alphabetical pick list is another common contributing factor of errors arising from look-alike drug names. An example from the ISMP MERP follows.
One hospital reported several mix-ups between injectable diazepam and diltiazem when removing the drugs from an ADC in the ICU. In each case, the nurse incorrectly chose diazepam on the screen, which was listed directly above the intended product, diltiazem. In one case, diazepam was given at the prescribed diltiazem dose. In another case, the error was discovered before it reached the patient when a physician noticed the amber colored vial and the product label was re-checked. It’s important to note that the nurses in these cases thought they had removed the correct product from the ADC. Thus, they failed to inspect the product label carefully, missing opportunities to catch the original selection error. A way to guard against this predictable failure is to ensure that ADC cabinets are interfaced with the pharmacy computer so they do not allow access to drugs that do not appear on a patient’s profile.
Quantity of drugs. ADCs that contain a wide assortment or excessive quantities of medications can also increase the risk of errors, like the colchicine incident above, especially if the ADCs are not profiled to the pharmacy computer. The following example, from the ISMP MERP, shows the safety net that carefully limited ADC stock can offer.
After the pharmacy was closed, an order was written for “1 gram calcium gluconate IV.” Each 10 mL vial contains 1 g of calcium gluconate, which is equivalent to 93 mg of elemental calcium. The nurse misunderstood this information on the label and thought she needed about 10-11 vials to prepare the 1 g dose. Luckily, the ADC contained only six vials. The ten-fold error was discovered and averted when the nurse contacted a pharmacist about the need for additional vials.
Stocking processes. Stocking medications in ADCs is primarily a pharmacy function, although nurses may return unused doses to an ADC—an error-prone practice we do not endorse. Cabinets that do not employ bar-coding technology rely on a double-check system before the medications leave the pharmacy. This process is vulnerable to errors because there is rarely any system used to verify that the correct drug has been placed in the correct drawer. Recall the well-publicized infant deaths when vials of heparin 10,000 units/mL were misplaced in a pocket meant for heparin 10 units/mL. Other examples submitted to PA-PSRS and ISMP MERP involved erroneous stocking of the following drugs or strengths, many with look-alike drug names or packaging:
- NUBAIN (nalbuphine) in an adjacent drawer intended for BUPRENEX (buprenorphine)
- FIORICET (acetaminophen, butalbital, caffeine) in a drawer intended for FIORINAL (aspirin, caffeine, butalbital)
- HYDROmorphone 4 mg syringes in a drawer intended for morphine 4 mg syringes
- tiZANidine (ZANAFLEX) in the compartment intended for tiaGABine (GABITRIL)
- Abbott Carpuject syringe of digoxin in the drawer intended for ketorolac.
Storing medications with look-alike names and/or packaging next to each other in the same drawer or bin has also contributed to stocking and retrieval errors, particularly during emergencies when the patient profiling system is bypassed. An example of this type of error reported to PA-PSRS follows.
During a cardiac catheterization, a nurse received a verbal order for IV LOPRESSOR (metoprolol). She accidentally removed LEVOPHED (norepinephrine) from the ADC, which was stored in a bin adjacent to Lopressor. The patient received the incorrect medication and required treatment and observation during and after the procedure.10
ADC Safety Recommendations
Before ADCs, technicians prepared doses, pharmacists checked their work, and the medications were dispensed to patient care units in carts or placed in nurse servers. Nurses then served as a final independent check of the dispensed medications. With ADCs, if medications are stocked and removed without bar-coding, the same level of redundant check systems no longer exists, even when the pharmacist verifies the medication order before the nurse can access the medication. Therefore, it is crucial to use ADC systems with minimal bypasses so that safety is on par with other methods of dispensing unit-dose medications, such as robotic dispensing or manual cart fills, which include several built-in redundancies.
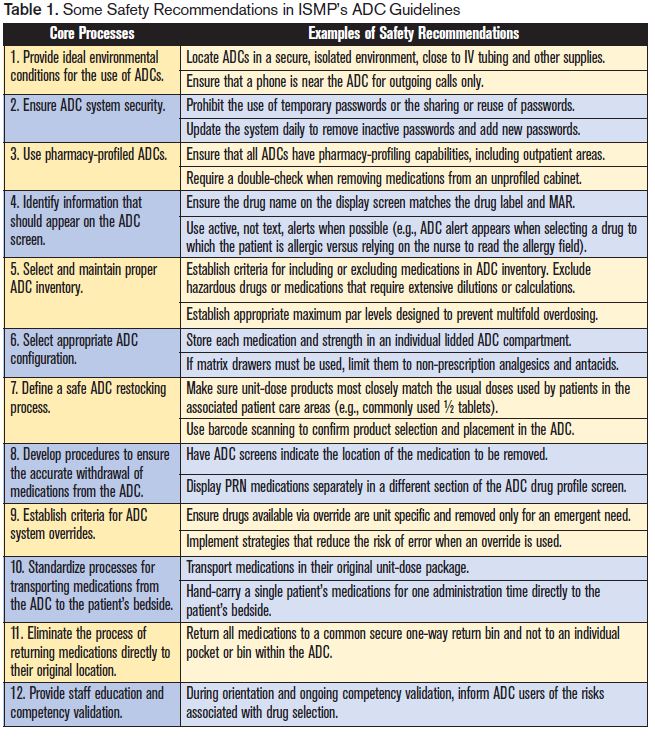
In spring 2007, ISMP convened a national forum of stakeholders to develop interdisciplinary guidelines for promoting safe practices when employing ADC technology. The guidelines were finalized in March 2008. A few examples from each of the 12 core processes described in the guidelines are included in Table 1. The immediate implementation of all elements in the guidelines is an ambitious goal, but there are things you can do today to improve safety with ADCs. The guidelines are meant to support organizations (and vendors) in making resource and strategic planning decisions as well as facilitating ongoing safety enhancements.
Last week, Cardinal Health’s Center for Safety and Clinical Excellence sponsored a webcast on Best Practices for Automated Dispensing Cabinets, in which ISMP participated. We are also happy to announce that we have nearly completed a self-assessment for ADC technology, which we will make freely available on our website to all healthcare providers by the end of March. We encourage all organizations that employ ADCs to form interdisciplinary teams to review the guidelines, listen to the webcast, and complete the self-assessment to maximize safety.
References
- Pedersen CA, Gumpper KF. ASHP national survey on informatics: assessment of the adoption and use of pharmacy informatics in US hospitals—2007. Am J Health-Syst Pharm 2008;65(23):2244-64.
- Oren E, Shaffer ER, Guglielmo BJ. Impact of emerging technologies on medication errors and adverse drug events. Am J Health-Syst Pharm 2003;60:1447-58.
- Klein EG, Santora JA, Pascale PM et al. Medication cart-filling time, accuracy, and cost with an automated dispensing system. Am J Hosp Pharm 1994;51: 1193-6.
- Ray MD, Aldrich LT, Lew PJ. Experience with an automated point-of-use unit-dose drug distribution system. Hosp Pharm 1995;30(1):18,20-3,27-30.
- Borel J, Rascati K. Effect of an automated, nursing unit-based drug-dispensing device on medication errors. Am J Health-Syst Pharm 1995;52:1875-9.
- Shirley KL. Effect of an automated dispensing system on medication administration time. Am J Health-Syst Pharm 1999;56:1542-5.
- Schwarz H, Brodowy B. Implementation and evaluation of an automated dispensing system. Am J Health-Syst Pharm 1995;52:823-8.
- Barker K, Pearson RE, Hepler CD et al. Effect of an automated bedside dispensing machine on medication errors. Am J Hosp Pharm 1984;41:1352-8.
- Shojania KG, Duncan BW, McDonald KM, et al. eds. Making Health Care Safer: A Critical Analysis of Patient Safety Practices. Evidence Report/ Technology Assessment No. 43 (Prepared by the University of California at San Francisco-Stanford Evidence-based Practice Center under Contract No. 290-97-0013), AHRQ Publication No. 01-E058, Rockville, MD: Agency for Healthcare Research and Quality. July 2001.
- Pennsylvania Patient Safety Authority. Problems associated with automated dispensing cabinets. Patient Safety Authority. 2005; 2 (3): 21-23.