
Fatal Overdose Uncovers Need to Rethink Where Pediatric IV Medications Are Dispensed and Administered
Problem: In October 2007, Florida news media reported a tragic, fatal medication error involving a 3-year-old boy who received a 10-fold overdose of arginine (R-GENE 10, 10% arginine hydrochloride injection) during an outpatient growth hormone stimulation test.1-3 Even though the child’s mother had questioned the dose, and his father had asked that the procedure be stopped when his son exhibited symptoms of distress, the error was not detected until the next day, after the child was hospitalized and declared brain dead.
Before the test, the child’s parents had taken him to a physician because he was small for his age. He was subsequently scheduled for a diagnostic test at a pediatric clinic to assess his pituitary function. The test involved the IV administration of the amino acid arginine, which stimulates pituitary release of growth hormone and prolactin through origins in the hypothalamus. Patients with impaired pituitary function will exhibit no increase or a lower than expected increase in plasma concentrations of growth hormone after administration of arginine. The test is a useful diagnostic aid in such conditions as craniopharyngioma, hypophysectomy, pituitary trauma, acromegaly, gigantism, and problems of growth and stature.
The child’s physician had prescribed 5.75 g of arginine (500 mg/kg/dose for the 11.5 kg child) to be administered IV over 30 minutes, but the child received 60 g in error. An outpatient pharmacy had dispensed the drug. R-Gene 10, the only brand of arginine available in the US, is supplied in 300 mL bottles containing 30 g each—the recommended dose for an adult undergoing testing. Smaller containers are not available for pediatric patients.
The child’s parents had been given a prescription for arginine to take to a community pharmacy to be filled. The pharmacy did not carry the drug, so the parents returned to the clinic to find out how to have it dispensed. The clinic nurse phoned in a prescription for arginine to an outpatient pharmacy associated with the clinic. The product was not in stock in this pharmacy either, so the pharmacist jotted down a note on the prescription that said “2 bottles” to remind her to order 2 bottles of the drug. The use of arginine to test pituitary function had increased recently, and she wanted to keep a bottle in reserve for the next scheduled test. Later, the prescription was entered into the computer by a second pharmacist who misinterpreted the notation of “2 bottles” on the prescription to mean that the test was going to be performed on one day and repeated on another day. The second pharmacist thought the parents wanted to pick up both bottles at the same time.
On the day of the test, both bottles were dispensed to the parents, each labeled, “Take to clinic and infuse 5.75 gm.” The pharmacist had also marked each bottle on the corner of the label as “1 of 2” and “2 of 2” to identify that more than a single container was to be picked up by the parents. However, the clinic staff thought that both bottle # 1 and bottle # 2 were required to administer the prescribed dose.
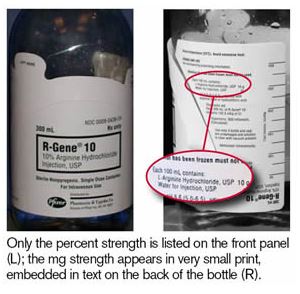
The nurse who administered the drug read the pharmacy labels on the bottles and thought that, together, the dose would equal 5.75 g. (The nurse had made a similar error before, believing that the entire bottle dispensed from the pharmacy contained the patient-specific dose; in that case, the child experienced adverse effects but recovered without permanent harm. This prior error was detected while investigating the more recent event.) The manufacturer’s labeling on the front of the bottle prominently displays the brand name, generic name, and percent concentration of 10% (see Figure 1). However, the strength (10 g/100 mL) only appears in very small print on the back of the bottle, which the nurse failed to see. The nurse did not recognize that each bottle contained 30 g of arginine, nor was she alerted to the error by the extremely rapid rate of infusion (1,200 mL/hour) required to administer the drug over 30 minutes, as prescribed.
Before the infusion, the child’s mother asked the staff to check the dose; she was assured it was correct. When the child developed signs of distress, including a severe headache, the father asked to halt the procedure. A physician checked the child’s medical records for the prescribed dose and asked the nurse how much medication he had received. The nurse responded that “75%” of the medication had infused, never mentioning the actual dose. Finding no reason to stop the test, the physician ordered continuation of the infusion without visualizing the actual bottle(s) of medication. Upon completion of the infusion, the child was discharged. That night, he was brought to the emergency department, disoriented and vomiting, and admitted to the hospital for dehydration. The next day, the parents continued to report that their child was not “acting normally.” That evening, after a witnessed seizure, the child was transferred to a pediatric ICU at another hospital. He was later declared brain dead, and his parents were informed about the medication error.
Under the WARNINGS section of the package insert for R-Gene 10, the manufacturer, Pfizer, acknowledges that two reports of possible overdoses in children were reported before this event occurred. The warning states: Extreme caution must be exercised when infusing R-Gene 10 into pediatric patients. Overdosage of R-Gene 10 in pediatric patients can result in hyperchloremic metabolic acidosis, cerebral edema, or possibly death.
Safe Practice Recommendations
This tragic error might have been avoided or detected earlier had any one of five key error-reduction strategies been in place:
- dispensing and administering IV drugs to children according to established protocols in dedicated infusion centers where pharmacy and nursing staff are likely to be more familiar with the administration of arginine,
- dispensing patient-specific doses of pediatric IV medications,
- requiring an independent double-check of IV pediatric medications, particularly hypertonic IV solutions,
- maintaining a heightened index of suspicion of error based on expressed patient/family concerns, and
- changing the manufacturer’s label on the product to make the strength (30 g/300 mL) clearly visible on the front panel.
Dedicated infusion centers and protocols. The organization where the event occurred now restricts the administration of IV pediatric solutions/medications to dedicated infusion centers rather than clinic areas. While the outpatient pediatric clinic where this error happened was likely staffed with well-qualified practitioners, an additional level of safety might be attainable in a setting where: 1) standardized practices for IV infusions are well integrated and consistently carried out, 2) pharmacy and nursing staff are more familiar with the types of medications most commonly administered, 3) pharmacy staff possess the experience and equipment to prepare and dispense IV infusions, and 4) protocols have been established and are referenced during testing and drug administration. Additionally, access to a pharmacist for questions might be more readily available in a dedicated infusion center.
Dispensing patient-specific doses. Pfizer does not offer R-Gene 10 in smaller volumes more appropriate for pediatric doses; the drug is only available in a unit-dose container for adults. Thus, arginine prescriptions for pediatric patients should be dispensed from pharmacies that are: 1) staffed with pharmacists who are experienced in preparing pediatric IV infusions, 2) furnished with the equipment necessary to prepare patient-specific IV doses, and 3) able to dispense the drug to the infusion area immediately before use. Full bottles from the manufacturer should never be dispensed for pediatric patients, even with directions for use on the label. Pfizer has been contacted several times to request information about stability of the drug once it is removed from its original container, as there is no information about this in the package insert. A company representative informed us that stability has not been tested, but he referred the question to another department, and we have not yet received a call back. We believe it would be safest (unless we hear otherwise from the company) to withdraw the prescribed amount of drug from the manufacturer's glass bottle and inject it into a smaller, evacuated sterile glass bottle with a label that includes the dispensing time and a prominent note to "begin administration within 30 minutes of dispensing."
Independent double-checks. It is uncertain whether an independent double-check in the pharmacy prior to dispensing the drug would have detected the dispensing error (2 bottles). However, patient counseling at the point of sale might have brought attention to the fact that the child was not scheduled for more than one test. The dispensing error also might have been detected if the nurse who administered the medication had asked another nurse to check the drug and dose/infusion rate. Arginine should always be independently double-checked before dispensing and administration, particularly since it is hypertonic (950 mOsmol/L) and contains 47.5 mEq of chloride ion per100 mL of solution (compared to 308 mOsmols/L and 15.4 mEq of chloride per 100 mL of 0.9% isotonic sodium chloride).
Heightened suspicion of an error. One of the most regrettable aspects of this tragedy is that the concerns expressed by the child’s parents about the dose, and their son’s reaction to the test, did not lead to early detection of the error. Without knowing all the facts in this case, we assume that the nurse who administered the medication and the physician who later examined the patient during the test took the parents’ expressed concerns seriously and rechecked the testing procedure. Nevertheless, this case clearly illustrates that our index of suspicion of an error should be very high when patients or family members speak up about medication safety concerns.
Manufacturer labeling. We have contacted Pfizer and FDA to express our concerns about the labeling of the product’s strength. We suggested listing the product’s strength (30 g/300 mL) directly under the product name on the front panel. We are awaiting a response from the company.
We applaud and support the leaders in the facility where this error happened for their honest disclosure of the event to the child’s parents, sincere public statements of apology, and support of the family during this difficult time. The child’s family also has publicly expressed appreciation for the organization’s candor, ethical and thorough investigation of the event, and sincere condolences. The family has established a charitable foundation in their child’s name to support the establishment of a free-standing, state-of-the-art children’s hospital in Gainesville, FL.
References:
- Chun D. ...apologizes for death of boy. The Gainesville Sun, Oct. 26, 2007.
- Tasker F. Toddler’s death leads to stricter medical safeguards. Miami Herald, Oct. 27, 2007:A1.
- Associated Press. Medication error causes death of boy, 3. Florida Today, Oct.25, 2007.