
Fatal Outcome After Inadvertent Injection of Topical EPINEPHrine
Problem: A patient in Canada recently died after receiving an injection of epinephrine 1:1,000 from a syringe that a surgical nurse and surgeon thought contained a local anesthetic. Staff at the hospital where the event happened worked collaboratively with ISMP Canada to issue a country-wide bulletin to draw attention to the tragic event and encourage a call to action for all hospitals to prevent similar errors. ISMP Canada has allowed us to share the information which appeared in the March 5, 2009 issue of the ISMP Canada Safety Bulletin with US hospitals, because a similar event could happen here.
Description of the Event
During a procedure, a surgeon requested lidocaine 1% with EPINEPHrine 1:100,000 for injection as a local anesthetic and was handed a syringe containing what he thought was the requested medication. The surgeon injected the medication into the surgical site. Immediately afterward, the patient experienced a cardiac arrhythmia leading to cardiac arrest. Despite full resuscitation measures, the patient died. Information gathered after the event indicated that the syringe contained EPINEPHrine 1 mg/mL (1:1,000) intended for topical use.
Similar Prior Event
You may recall a similar event that occurred more than a decade ago in the US in which a 7-year-old boy died during a tympanomastoidectomy after receiving a fatal dose of EPINEPHrine (ISMP Medication Safety Alert! Case update: EPINEPHrine death. December 4, 1996). In the 1996 case, EPINEPHrine 1:1,000 was accidentally poured into a cup on the sterile field labeled “lidocaine with EPINEPHrine.” This cup should have been used for soaking pledgets (type of sterile gauze packing) with EPINEPHrine, but they were never added. The surgical technician drew 3 mL from the cup labeled lidocaine with EPINEPHrine, but the syringe actually contained 3 mg of EPINEPHrine. That syringe was used to infiltrate the ear, causing the child’s cardiac arrest.
Contributing Factors
The most recent event differs from the event described in our December 4, 1996 newsletter. In the earlier case, EPINEPHrine had been poured into a bowl labeled “lidocaine with EPINEPHrine.” In the recent event, EPINEPHrine had been drawn into a syringe and mistaken as the local anesthetic to be injected.
EPINEPHrine 1 mg/mL for topical use was on backorder in the pharmacy, so epinephrine 1 mg/mL for injection was provided for use in the operating room (OR). As a result, the nurse used a needle and syringe to withdraw the contents from the vial, rather than directly pouring the EPINEPHrine from the manufacturer’s container into the sterile open container with the pledgets. The syringe containing epinephrine 1 mg/mL was not labeled.
Usually, the topical EPINEPHrine and local anesthetic for injection were prepared before the start of the procedure. But the OR nurse was interrupted after drawing the EPINEPHrine 1 mg/mL into a syringe, so she placed it on the back table. Later, when the surgeon requested the local anesthetic for injection, the nurse placed the EPINEPHrine (1 mg/mL) syringe on the stand beside the OR table, believing it contained the injectable anesthetic.
Safe Practice Recommendations
The most forthright recommendations to avoid an error like the most recent event are to always label syringes and containers, and discard unlabeled products. However, the event that occurred more than a decade ago involved a substitution error in which the topical EPINEPHrine was poured into a container labeled as lidocaine and EPINEPHrine. Thus, all facilities that perform procedures requiring the use of EPINEPHrine 1 mg/mL (1:1000) for topical application should review their processes and consider the following recommendations.
Differentiate. Always supply epinephrine for topical use in a pour-bottle (vial with peel off cap). If pour-bottles from manufacturers are not available (e.g., backorder), require pharmacy to prepare ready-to-use doses in pour-bottles or topical syringes, and to communicate the expected change in appearance to all affected service areas. Never take the risk of withdrawing a topical medication into a parenteral syringe.
Provide label clarity. Ensure that the word “TOPICAL” appears on the label of any container used to hold a solution intended for topical application.
Distinguish processes. Develop distinct processes for preparing and handling EPINEPHrine for topical application. In particular, medications such as EPINEPHrine intended for topical application should not be placed into a parenteral syringe. Conversely, a medication intended for injection (e.g., local anesthetic) should not be placed into an open container.
Separate processes. Store and prepare medications intended for topical use in distinctly separate areas from those used for storing and preparing medications for injection. Some surgeons also infiltrate (i.e., inject) the surgical site with local anesthetic before scrubbing and gowning for ear, nose, and throat procedures. Subsequent infiltration is seldom needed, but if required, additional local anesthetic should be withdrawn directly from the vial.
Verification. Keep local anesthetics for injection in their original vials, and withdraw the medications into a syringe (and label it) immediately before use. This allows the surgeon to verify the drug by comparing the vial and syringe label.
Simplify. If possible, replace the need for vials of topical EPINEPHrine with presoaked EPINEPHrine pledgets prepared in advance of procedures.
Limit access. Do not stock multiple-dose vials of injectable EPINEPHrine 1 mg/mL in the OR, which look very similar to the 30 mL vials of topical EPINEPHrine.
Although not directly related to the most recent fatality, practitioners in the US and Canada have often expressed concerns about similarities between the pour-bottles of topical EPINEPHrine and vials of injectable medications (see Figures 1 and 2). 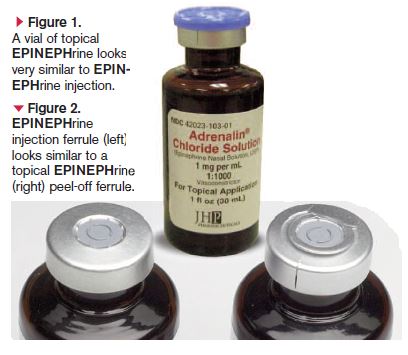 The pour-bottles have a rubber stopper held in place by a metal ferrule and a tab which, when pulled, removes the metal ferrule, yielding a “pour-bottle” format. However, the rubber stopper and metal ferrule give the pour-bottle an appearance very similar to a vial of injectable medication. The similarities have led to mix-ups between local anesthetics with EPINEPHrine and vials of topical EPINEPHrine. The rubber stopper has also encouraged some practitioners to use a parenteral needle and syringe to with-draw the topical EPINEPHrine. ISMP and ISMP Canada have alerted the manufacturers to the potential risks associated with the packaging of the pour-bottles of topical EPINEPHrine.
The pour-bottles have a rubber stopper held in place by a metal ferrule and a tab which, when pulled, removes the metal ferrule, yielding a “pour-bottle” format. However, the rubber stopper and metal ferrule give the pour-bottle an appearance very similar to a vial of injectable medication. The similarities have led to mix-ups between local anesthetics with EPINEPHrine and vials of topical EPINEPHrine. The rubber stopper has also encouraged some practitioners to use a parenteral needle and syringe to with-draw the topical EPINEPHrine. ISMP and ISMP Canada have alerted the manufacturers to the potential risks associated with the packaging of the pour-bottles of topical EPINEPHrine.
ISMP thanks ISMP Canada and the involved hospital for sharing this story with readers of this newsletter.