Error-prone Conditions that Lead to Student Nurse-Related Errors
If your organization provides a site for clinical rotations of student nurses, you are probably aware that students can be involved in medication errors despite close supervision by their clinical instructors. When analyzing errors involving student nurses reported to the USP-ISMP Medication Errors Reporting Program and the PA Patient Safety Reporting System, it appears that many of the errors arise from a distinct set of error-prone conditions or medications. Some student-related errors are similar in origin to those that seasoned licensed healthcare professionals make, such as misinterpreting an abbreviation, misidentifying drugs due to look-alike labels and packages, misprogramming a pump due to a pump design flaw, or simply making a mental slip when distracted. Other errors stem from system problems and practice issues that are rather unique to environments where students and hospital staff are caring together for patients.
The duality of patient assignments is a prime example. Patients who are assigned to student nurses are also assigned to staff nurses. While dual assignments are necessary, communication breakdowns regarding who will administer the prescribed medications to patients, what medications have been administered, and which medications should be held, have resulted in dose omissions and the administration of extra doses. Thus, the communication between students, nursing instructors, and staff needs to be planned carefully to ensure a model that considers the safety issues associated with dual assignments.
Data from the reporting programs also show that insulin is among the most frequent drugs involved in student nurse-related errors, particularly with omitting prescribed doses, selecting the wrong type of insulin, administering the wrong sliding-scale insulin coverage, and administering insulin to the wrong patient. Student nurses may not make proportionately more errors with insulin than staff nurses. However, like staff nurses, students and nursing instructors must treat insulin as a high-alert medication and observe the robust safeguards in place to prevent errors. This should include an independent double-check of all insulin doses by a staff nurse before administration. Additionally, organizations should share their list of high-alert drugs and associated error-reduction strategies with nursing instructors to ensure the same level of attention to safe systems and practices occurs when students administer these drugs.
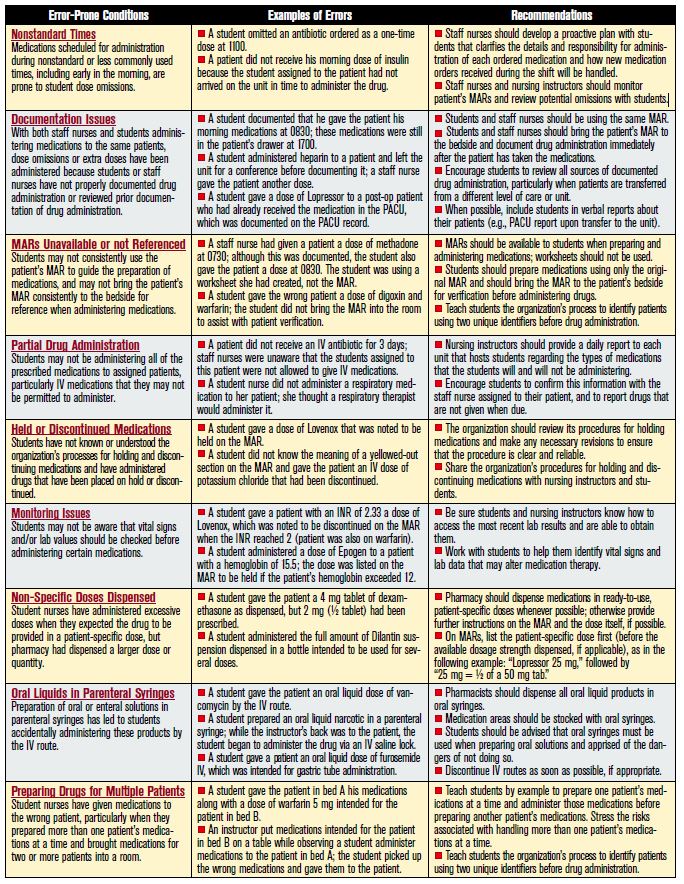
In Table 1 we have listed additional error-prone conditions identified through analysis of student nurse-related errors. The list is not intended to be critical of student nurses or their instructors, nor is it intended to discourage organizations from providing a clinical rotation site for students. Indeed, student nurses often enrich the patient’s experience during hospitalization, and they should be welcomed as part of the patient care team. Rather, the information in Table 1 should be used to stimulate system improvements to reduce the risk of medication errors.
Each practice site that hosts student nurses should meet with the clinical instructors who will be supervising students. The organization’s medication administration procedures and specific error-prone conditions that may exist during clinical rotations should be reviewed, along with system-level safety nets that have been designed to reduce these risks, and safety practices that students and faculty should adopt to further enhance patient safety. In addition to the examples in Table 1, nursing instructors may be able to describe other error-prone conditions that they have observed, which can then be addressed. Nursing instructors should also be invited to attend any orientation programs that cover the organization’s safety goals so they can reinforce related safe practices during clinical rotations.