
COVID-19-Related Medication Errors
In our April 9, 2020 newsletter, we shared an idea to add a question, “Is this event related to COVID-19 (coronavirus)?” to reporting systems to categorize COVID-19-related events, allow rapid analysis of quickly emerging risks, and reduce leadership’s reaction time in knowing about and addressing some of these issues. Since then, we have received several COVID-19-related medication errors each week and wanted to update you on a few important issues.
Remdesivir investigational drug labeling confusion
ISMP received a report last week about a hospital compounding issue due in part to label confusion with the investigational drug remdesivir. Some facilities have received this drug, manufactured by Gilead Sciences, under a compassionate use program during a period of expanded access and through an emergency use authorization (EUA) program issued by the US Food and Drug Administration (FDA). The hospital had implemented an investigational study using intravenous (IV) doses of remdesivir to treat patients with severe COVID-19. The adult protocol called for an initial loading dose of 200 mg, followed by subsequent 100 mg doses. Each vial of remdesivir contains a total of 100 mg. Instead of using 1 vial to prepare each 100 mg subsequent dose, 2 vials were used, thus providing 200 mg for each subsequent dose instead of the intended 100 mg.
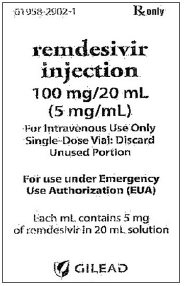
Remdesivir is available for use in clinical trials in at least two different dosage forms: a lyophilized powder for injection and a solution for injection. Like many investigational drug container labels, the vials are not clearly labeled, and the information presented is crowded and in a small font (see our 2-part article about problems with investigational drug labeling: Part I - April 19, 2018; Part II - May 3, 2018). The vials of lyophilized powder have a label listing the total amount (100 mg) of drug in the vial (Figure 1). The vials of remdesivir injectable solution have a label that lists the per mL strength, “Remdesivir (GS-5734) Injection, 5 mg/mL” (Figure 2). Below the 5 mg/mL listing, the vial label notes the total volume in the vial, “Contents: 21.2 mL,” which may be easy to miss. Another label presentation is available for the remdesivir injectable solution, which lists the total dose per total volume first (100 mg/20 mL), with the per mL amount (5 mg/mL) in parentheses below it, as per USP <7> (Figure 3). The hospital where the error happened only had remdesivir with the first two label presentations in stock (Figures 1 and 2); pharmacy staff were using the remdesivir injectable solution (Figure 2) when the error occurred.
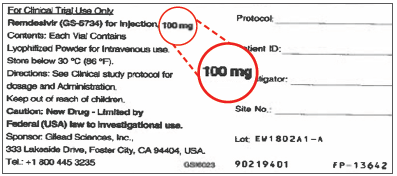
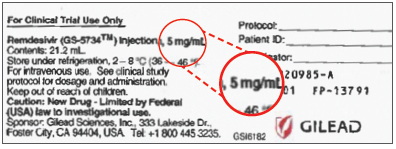
The hospital identified that at least two factors contributed to the compounding error. First, there was initial confusion with the labeling of the injectable solution vial, which does not include the total dose (100 mg) contained in the vial (Figure 2). Second, confirmation bias played a significant role in the error. The technician inadvertently used 2 vials to prepare each subsequent remdesivir dose, exactly as he had just done minutes before when preparing several loading doses. A pharmacist failed to catch the error during the checking process (there was no barcode available to scan on the vials), and the erroneous 200 mg doses (which were labeled as 100 mg doses) were administered to multiple patients that day. No adverse reactions have been reported at this point. Reconciliation in the pharmacy at the end of the day for all remaining remdesivir vials, which was performed similar to a narcotic inventory reconciliation, led to identification of the error.
To prevent errors, consider adding a printed barcode label to each remdesivir container so barcode scanning can be used for product and dose verification. If you stock the vials seen in Figure 2, pharmacies may also want to consider affixing an auxiliary label to remdesivir injectable solution vials to note the total amount of drug (100 mg) contained within. Also provide prescribers, pharmacy staff, and nurses with a Fact Sheet and/or Pharmacy Guide on remdesivir provided by the manufacturer. ISMP is in communication with Gilead about the label issue.
Failure to engage barcode medication administration (BCMA)
A hospital noticed that several COVID-19-related errors were undetected before reaching patients due to a failure to engage BCMA at the bedside. These errors were associated with COVID-19-induced staffing changes, which resulted in redeploying operating room (OR) nurses, who were not familiar with BCMA, to other patient care units. One error involved a redeployed OR nurse who administered an albuterol inhaler instead of the intended BREO ELLIPTA (fluticasone furoate and vilanterol) inhaler after failing to use the unfamiliar BCMA technology. The hospital learned that redeployed nurses require orientation to the patient population, technologies, processes, and medications typically used on the newly assigned unit.
Inability to weigh patients during telehealth encounters
An oncology clinic reported an unintended consequence of telehealth visits—the inability to document an accurate weight, leading to incorrect dosages of weight-based drugs. In this case, the patient had come into the clinic for her first chemotherapy treatment—protein-bound PACLitaxel and gemcitabine. Due to COVID-19, the patient had been participating in telehealth visits for several months prior to her first chemotherapy treatment, during which measured weights were not obtained or regularly updated. The patient’s weight had not been measured or updated for 4 months; however, a weight was obtained when she arrived at the oncology clinic for her first dose of chemotherapy.
Unfortunately, the current chemotherapy plan had been based upon the previous weight measured 4 months ago. The patient had lost substantial weight since that time, and while double-checking the chemotherapy dose, the nurse noticed that the patient’s body surface area (BSA) was 7% lower than the BSA listed on her chemotherapy treatment plan. In this organization, a BSA difference of 5% or greater requires a change in the dose; however, it took more than 2 hours to authorize a revised dose based on the patient’s current BSA, delaying the beginning of chemotherapy administration. The clinic is working on a process to flag weights in the electronic health record that require updating prior to prescribing, dispensing, and/or administering weight-based medications. The clinic staff are now inquiring about weight loss or gain during all telehealth encounters.
Entering just a few letters for an ADC drug name search leads to an error
In the intensive care unit, a 40-year-old intubated man with COVID-19 received verapamil instead of VERSED (a former brand of midazolam). The patient had become agitated, so the physician verbally asked a nurse to increase the dose-rate of the patient’s propofol infusion and to administer “Versed” 2 mg IV push. The nurse used the override feature in the automated dispensing cabinet (ADC) to select and access the drug “Versed” by entering the first few letters of the drug name. She accidentally selected and removed a vial of verapamil (5 mg/2 mL) from the ADC, which was available via override. The nurse administered verapamil IV push to the patient, believing it was “Versed.” She did not employ the available bedside barcode scanning system because the medication was a verbal order and had not yet been entered into the health record. About 15 minutes later, the nurse recognized the error when documenting administration. The patient was monitored and suffered no long-term harm from the error.
The hospital is now assessing its verbal order practices, intending to eliminate their use except in emergencies; examining its ADC override practices, intending to restrict their use; increasing the minimum number of letters used when searching for drugs in the ADC; and taking all the necessary steps to optimize the bedside barcode scanning system. In our Guidelines for Safe Electronic Communication of Medication Information, we recommend using at least 5 letters when searching for a drug in electronic systems. This error sounds eerily similar to a fatal ADC vecuronium-Versed mix-up, which was published in our January 17, 2019 newsletter. Please see that newsletter issue for recommendations related to limiting and monitoring ADC overrides and safe drug name searches.
Missed doses
One hospital analyzed numerous reports of missed medication doses for COVID-19 patients. Some reports involved missed doses of albuterol inhalers due to communication failures between nurses and respiratory therapists at the beginning of the COVID-19 pandemic. With improved communication strategies between departments, the issue has since been resolved. Other reports of missed doses related to the need to frequently enter patients’ rooms for drug administration. This resulted in further consolidation of standard medication administration times so that efforts to conserve personal protective equipment (PPE) and nurses’ time at the bedside could be continued.
Access this Free Resource
You must be logged in to view and download this document.