
California Department of Public Health Medication Error Reduction Plan
ISMP has long been an advocate for learning from the experiences of others—to take certain aspects of another’s experience and incorporate them into your own work and life for the purpose of improvement. It is in this spirit of learning that we share with readers our support of a state-wide initiative in California (CA) to reduce medication-related errors that can be used as an example for all US hospitals to voluntarily adopt a similar initiative.
As a condition of licensure, every general acute care hospital in CA was required to adopt a Medication Error Reduction Plan (MERP; not to be confused with the ISMP MERP [Medication Errors Reporting Program]) to substantially reduce medication–related errors by January 1, 2002. The plans were required to include the implementation of technology proven to reduce errors. The submitted plans were approved by the California Department of Public Health (CDPH), and each hospital was required to implement its plan before January 1, 2005. Each hospital must review and approve the plan annually.
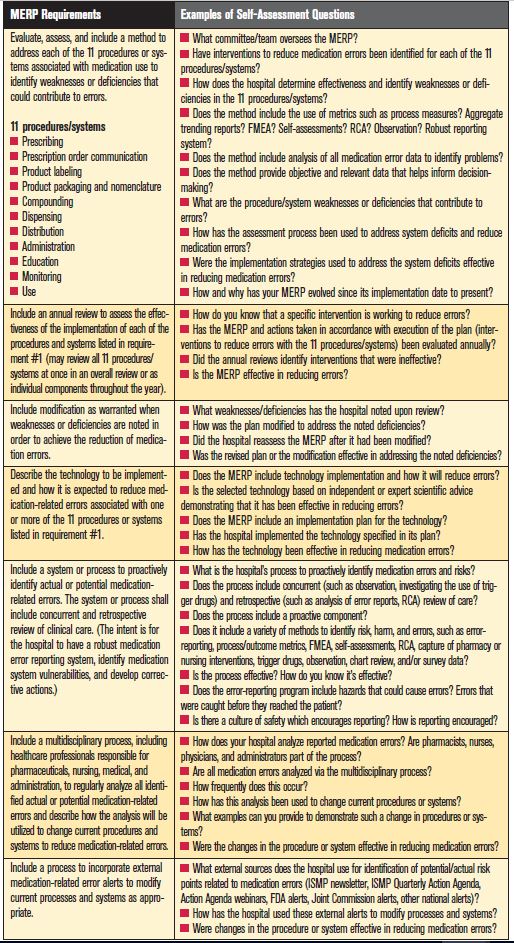
MERP Components
Details regarding the required components in the hospital’s MERP are provided in Table 1. In brief, each hospital must adopt a methodology to assess, improve, and evaluate medication safety, with particular attention paid to prescribing, prescription order communication, product labeling, product packaging and nomenclature, compounding, dispensing, distribution, administration, education, monitoring, and use. This methodology must include a system or process to proactively identify actual or potential medication-related errors as well as concurrent and retrospective review of clinical care. The regulation defines a “medication-related error” as any preventable medication-related event that adversely affects a patient and is related to professional practice or healthcare products, procedures, and systems, including but not limited to the elements listed above in bold text. A multidisciplinary process that includes pharmacists, nurses, physicians, and administrative leaders must be established to regularly analyze all identified actual or potential medication-related errors—not just aggregate reports about these conditions or events—and to use these findings to change current procedures and systems to reduce medication-related errors.
The MERP also must include plans for the implementation of technology and explain how it is expected to reduce medication errors (small and rural hospitals were exempt from implementing technology although many did not claim this exemption). Hospitals are required to conduct an annual review to assess the effectiveness of each of the 11 components of medication use (in boldface text above), and to make changes to interventions when weaknesses or deficiencies have been identified for the purpose of reducing medication errors.
Another essential feature of the CA MERP requires establishing a process to incorporate and learn from external medication-related error alerts, and to take action to modify current processes and systems as appropriate to reduce the risk of similar errors. Organizations cannot assume that systems are safe until proven dangerous by a tragic event. No news is not good news when it comes to patient safety. The regulation suggests that each organization needs to accurately assess how susceptible its systems are to the same errors that have happened in other organizations, and to acknowledge that the absence of similar errors is not evidence of safety. Personal experience is a powerful teacher, but the price is too high to learn all we need to know from firsthand experiences. Learning from the mistakes of others is imperative, and ISMP is especially supportive and pleased that the CA initiative requires this component in its MERP regulations.
Survey Findings
In January 2009, CDPH began conducting triennial onsite visits to monitor each facility’s implementation of its previously approved MERP. Of the 112 hospitals surveyed in 2009 (29% of all CA hospitals), 15% were following their approved MERP and 81% were deficient in implementing their plan. About half of the hospitals with deficiencies were cited for failing to establish and follow policies and procedures related to safe and effective systems for procurement, storage, and dispensing of drugs, or for not including physicians on the multidisciplinary team that reviews all medication-related reports. About a quarter of deficient hospitals were cited for failing to conduct an annual review to assess the effectiveness of the MERP itself and the error-reduction strategies in the plan, and/or for failing to identify weaknesses or deficiencies that could contribute to errors using both internal (e.g., hospital reporting program) and external (e.g., ISMP, FDA, Joint Commission) sources. In most cases, the deficiencies did not rise to the level of an “immediate jeopardy” to patients but instead required the hospital to establish an approved plan of correction.
Conclusions
ISMP supports the CA MERP initiative because it advances many of the error-reduction strategies we have supported over the years, including: a proactive approach to risk identification and analysis; carefully planned technology implementation; multidisciplinary teams to analyze medication-related risks and errors; use of external information to improve medication safety; effective and timely use of measurement/assessment systems to evaluate the impact of selected error-reduction strategies; and the design of an annually reviewed strategic plan to reduce medication errors. While we recognize significant resources and expertise are necessary to design and implement a robust MERP—coordination by a medication safety officer is highly recommended—we believe such an effort can significantly impact patient safety. We hope hospital leaders who work outside CA will provide the necessary staffing and resources to voluntarily establish a medication safety strategic plan in their hospitals with similar components. While we saw no mention in the CA regulations regarding a focus on high-alert medications and high-risk processes and populations, we encourage practitioners to devote their efforts on the drugs and processes that can harm vulnerable patients.
Requiring a multidisciplinary team to review all actual and potential medication-related errors individually may not be feasible in hospitals that have successfully increased the volume of error reports they receive, which often includes potential hazards and near misses. To require review of all medication-related errors could even discourage reporting. As an alternative, the team should establish error categories that should be reviewed individually (e.g., those that are more serious or have great potential for harm) while those less serious can be aggregated to work on as a whole (e.g., drug omissions which had no consequence). To do this, establish a system where data is prescreened by a medication safety officer or a similarly qualified professional to ensure that the multidisciplinary team is provided with the most relevant details about risks and errors that could lead to an adverse outcome in patients.
Next is the concern that regulatory agencies can sometimes become too prescriptive and/or too punitive when determining compliance with regulations. Indeed, we wrote about one such concern with CDPH and its citations in hospitals that had gone to great lengths to remove recalled drugs only to find supplies in unlikely places or from uncontrolled sources during a survey (Collaboration focused on priority issues promotes safety. ISMP Medication Safety Alert! Oct. 9, 2008). While we strongly oppose unreasonable sanctions of healthcare practitioners or too narrow assessment of healthcare providers that are meeting the intent of regulations, we must, however, support the CA MERP initiative to improve medication safety and encourage hospitals outside CA to adopt a similar program.
*Sources: Chapter 2.05 Minimization of Medication-Related Errors in the California Health and Safety Code Section 1339.63 (http://law.justia.com/california/codes/hsc/1339.63.html); All Facility Letter from CDPH issued on August 10, 2009 (www.cdph.ca.gov/certlic/facilities/Documents/LNC-AFL-09-31.pdf); All Facility Letter from CDPH issued on December 9, 2008 (www.cdph.ca.gov/certlic/facilities/Documents/LNC-AFL-08-39.pdf).