
Beware of Basal Opioid Infusions with PCA Therapy
Problem: A 63-year-old, 109 kg, opioid-naïve patient was admitted to a hospital with fractures sustained in a fall. She was given two doses of morphine 4 mg and one dose of HYDROmorphone 1 mg in the emergency department. Upon arrival to the inpatient unit, she was started on HYDROmorphone PCA (patient controlled analgesia), which included a basal infusion of 0.5 mg per hour, a demand dose of 0.2 mg with a lockout interval of 10 minutes, and a 4 hour limit of 6 mg. Continuous pulse oximetry was not in use. Five hours later, the patient was found unresponsive. Her respirations were six per minute, and her nail beds were beginning to turn blue. Oxygen saturation was checked with pulse oximetry and found to be 44%.
The rapid response team was called, oxygen was started, and two doses of naloxone were administered. In 15 minutes, the patient was alert and talking. It was then that the patient told a nurse she has sleep apnea and had previously used a continuous positive airway pressure (CPAP) machine at home. She hadn’t been using the CPAP recently. So, when the admitting nurse asked her if she used any medical equipment at home, she said “No.” The patient’s body mass index (BMI) was 38.6 (BMI of 40 or more is morbid obesity), placing her at risk for sleep apnea and hypoxemia during PCA therapy.
Although no permanent harm ensued, the hospital’s medication safety team used this case as a learning opportunity. Three root causes of the event were identified, as described below.
Dosing guidance. The PCA standard order form did not help guide prescribers to appropriate doses; instead, it provided a broad range of doses. For example, the range for a HYDROmorphone basal infusion dose was 0.1 to 0.5 mg/hour, and there was no guidance for selecting appropriate candidates for basal infusions. Many prescribers routinely selected a 0.5 mg/hour basal infusion, regardless of patient characteristics. A basal opioid infusion was not appropriate for this opioid-naïve patient.
Studies have shown that patients with basal opioid infusions are at least five times more likely to experience respiratory depression.1-4 The American Pain Society cautions against using continuous basal infusions because studies have failed to demonstrate significant differences in the quality of analgesia with or without basal infusions.4 There may also be an increased risk of programming errors when basal infusions are prescribed.5
Patient screening. The patient was not sufficiently screened for obstructive sleep apnea (OSA) and other risk factors for PCA-induced respiratory depression. The facility had an OSA screening process in place for pre-operative patients, but screening did not occur because this patient was not a surgical candidate.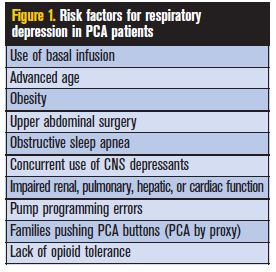 The incidence of respiratory depression in PCA patients ranges from 0.19 to 5.2 percent, depending on how it is measured.1-4 Figure 1 includes risk factors for respiratory depression in PCA patients.
The incidence of respiratory depression in PCA patients ranges from 0.19 to 5.2 percent, depending on how it is measured.1-4 Figure 1 includes risk factors for respiratory depression in PCA patients.
Patient monitoring. No process was in place to trigger an evaluation of the need for continuous pulse oximetry monitoring (or capnography for appropriate patients) during PCA.
Safe Practice Recommendations
The hospital’s medication safety team addressed these root causes by standardizing the PCA dosing process and revising the standard PCA order form as described below.
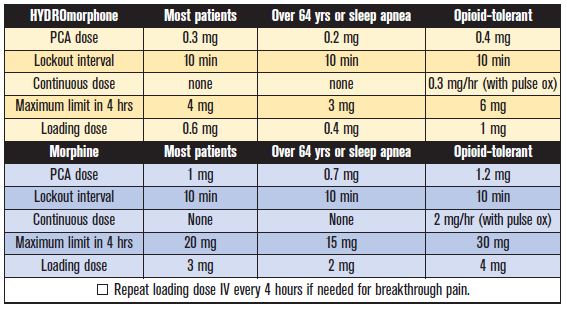
- Prescribers are guided to an appropriate dose based on age and opioid tolerance by providing default doses for three types of patients: most patients, patients over 64 years or with sleep apnea, and opioid-tolerant patients (see Figure 2).
- Basal infusions were eliminated except in opioid-tolerant patients.
- Basal infusions in patients with sleep apnea were prohibited.
- Opioid orders were rearranged to match the sequence in which the medications appear on the facility’s smart IV pumps.
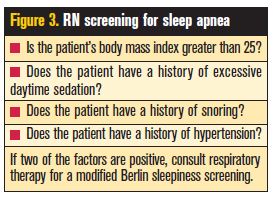
- A registered nurse is required to screen the patient for OSA before PCA initiation, with further assessment by a respiratory therapist if the screening shows two or more risk factors (see Figure 3).
- Continuous pulse oximetry (or capnography if appropriate) is required while on PCA if the patient has a continuous opioid infusion or sleep apnea, or if the patient is morbidly obese or older than 64 years.
- Patient education is required and must include instructions to the patient’s family not to push the PCA button for the patient (PCA by proxy).
The hospital also uses smart pumps for PCA therapy, with one standardized concentration for each drug and dose limits set in the pump library. Before converting to smart pumps, two PCA programming errors had occurred in recent years, leading to serious respiratory depression. Vast improvements in programming accuracy have been reported since switching to the smart pumps.
In our February 22, 2007 newsletter, we recommended avoiding basal infusions unless the patient is opioid-tolerant. Unfortunately, the term “opioid-tolerant” is not well understood. It is defined as “those patients who have received opioids regularly for approximately 7 days or more.” Opioid-naïve patients who present with high opioid requirements may be an exception and require a basal infusion, but additional safety steps should be instituted under these conditions. Our July 24, 2003, newsletter includes many recommendations to improve PCA safety, including the following.
- Evaluate the patient’s level of pain, alertness, and vital signs, including rate and quality of respirations, every 2-4 hours.
- Evaluate patients with minimal verbal and tactile stimulation to obtain an accurate assessment of their level of sedation.
- Monitor patients more frequently during the first 24 hours and at night, when hypoventilation and nocturnal hypoxia may occur.
- Employ early warning devices such as apnea alarms at night and pulse oximetry or capnography, which can alert practitioners to respiratory insufficiency.
Additional recommendations related to safe PCA use can be found in our July 24, 2003 newsletter.
References
- Hagle ME, Lehr VT, Brubakken K, Shippee A. Respiratory depression in adult patients with intravenous patient-controlled analgesia. Ortho Nurs 2004;23:18-29.
- McCaffery M, Pasero C. Pain: Clinical Manual (2nd ed.). Boston: Mosby, 1999.
- Weber L. Implementation of standard order sets for patient controlled analgesia. Am J Health-Syst Pharm 2008;65:1184-91.
- Principles of Analgesic Use in the Treatment of Acute Pain and Cancer Pain (5th ed.). Glenview, IL: American Pain Society, 2003.
- Ashburn M, Love G, Pace N. Respiratory related critical events with patient-controlled analgesia. Clin J Pain 1994;10:52-56.