
Analysis of Paramedicine Medication Errors Uncovers Challenges and Opportunities for Improvement
Paramedicine encompasses the provision of prehospital and out-of-hospital emergency, urgent, and preventive medical care delivered primarily by emergency medical services (EMS) providers, including emergency medical technicians (EMTs) and paramedics.1 As such, paramedicine includes the emergency assessment, treatment, and transport (by ground or air) of sick and injured patients, sometimes during life-or-death situations. During medical emergencies, EMS providers operate with medical oversight, either directly through a medical command center or by protocols developed by physicians experienced in emergency care. However, the uncontrolled prehospital setting, the time-sensitive nature of emergency patient care, and the rapidly changing status of ill or injured patients provide unique challenges that increase the risk of adverse events, including those caused by medication errors. For example, EMS providers often work in a small, crowded, poorly lit environment that is chaotic and loud, and they often have limited patient information upon which to make rapid, coherent clinical judgments.2 The environment may be further complicated by distractions, uncontrolled movement of people and vehicles, panicked family members, and curious bystanders.
Earlier this year, ISMP Canada published a multi-incident medication error analysis of about 60 paramedicine events reported to several Canadian reporting programs between 2000 and 2018 to identify themes relating to medication errors, describe the challenges associated with these themes, and highlight opportunities for improvement.3 In the US, medication errors occurring in the EMS prehospital setting have been significantly underreported to the ISMP National Medication Errors Reporting Program (ISMP MERP). Given the short interval of prehospital emergency care and the inability to follow-up regarding patient outcomes, EMS providers may not even be aware that a medication error has occurred. Despite minimal reports, ISMP reviewed 20 additional EMS-related medication errors submitted to the ISMP MERP between 2000 and 2019. The key findings and themes emerging from analysis of the Canadian and US events follow.
ERROR TYPES, DRUGS, AND HARM
About half of all Canadian incidents included in the analysis by ISMP Canada,3 and about three-quarters of all US incidents from the ISMP MERP, occurred during the administration stage of the medication-use process. The most common incident types were dose omissions, incorrect infusion rate or frequency of drug administration, incorrect drug, and dosing or mixing errors. Many of the incidents involved medications used to treat hypotension or shock, medications used during rapid sequence intubation, and opioids, particularly fentaNYL and morphine. Overall, approximately 1 in 5 reported EMS-related medication errors resulted in patient harm, which ranged in severity from mild (e.g., extravasation) to life-threatening (e.g., respiratory arrest).
THEMES
Analysis of the 80 events revealed four themes (one of which was further divided into three discrete subthemes) associated with EMS-related medication errors.3 These themes loosely follow the elements of the EMS response process.
Theme 1: Medication Errors Related to Clinical Assessment and Management
Challenges: When EMS providers reach the site of an emergency, there is often limited time for them to assess the ill or injured patient(s), gather relevant information, and evaluate the clinical concern. The providers must often rapidly determine their course of action, according to established protocols, guidelines, and treatment options. Incoherent or unconscious patients may not be able to provide important information about their disease processes or traumatic injuries. Their caregivers, if available, may not effectively communicate crucial information about the patients. Given the urgency of certain situations and the lack of access to key data (e.g., test results), information gathering (e.g., past medical history, medication use) and assessment may be incomplete, which can compromise treatment decisions.
Example: A patient who was experiencing pain at home called 9-1-1 and self-applied two fentaNYL transdermal patches (50 mcg/hour) before EMS arrival and transport. In the ambulance, the patient was given another opioid, morphine 2 mg intravenous (IV) push. At the hospital, the patient’s pain appeared to be inadequately controlled, and the physician ordered yet another opioid, HYDROmorphone 1 mg IV push. The patient was later found unresponsive and experiencing respiratory depression. Neither the EMS providers nor the hospital staff had asked the patient about prior opioid use. Therefore, they were unaware that the patient had previously been using fentaNYL patches but had discontinued the medication months earlier. They were also unaware that the patient had applied two leftover fentaNYL patches (under his clothing) before EMS arrival.
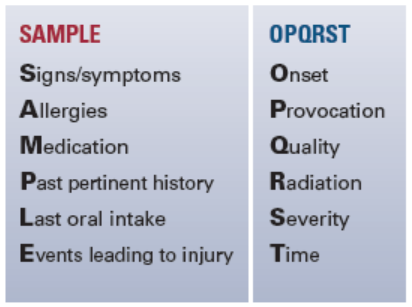
Opportunities for Improvement: When caring for any EMS patient, it is important to ascertain the complete medical history, including current medication use and clinical findings, and to communicate these details to other healthcare practitioners involved in the patient’s care when possible. EMS providers should always ask for the patient’s complete list of current home medications, as this list serves as an important source of medication information that can be communicated to other healthcare practitioners.2 Also, communicating with caregivers or family members, if available, can help gain a better understanding of the patient’s medical history, current condition, and recently taken medications, thus improving the quality of clinical judgments and reducing the risk of medication errors. It may also be helpful to reinforce a standard methodology for collecting information about patients (Figure 1) and to provide standardized patient information collection forms to prompt for important information, such as allergies, height and weight (in kg), pregnancy/breastfeeding status, presence of medication patches, and current lab results.
Theme 2: Medication Errors Related to Therapeutic Product Use
After assessing the patient, EMS providers will often administer medications and/or hydrating solutions to the patient in a chaotic and hurried environment at the scene and/or during transport. The equipment, medications, and solutions they use are often provided in compact bags, boxes, backpacks, or storage pockets (Figure 2) rather than in well-labeled and automated storage locations. This limitation reduces the opportunity to organize and label equipment, medications, and solutions optimally, increasing the risk of medication errors. Three subthemes related to therapeutic product use were identified.

Subtheme 1: Unclear Medication Labeling and/or Packaging
Challenges: The labeling and/or packaging of medications, such as look-alike product names or packaging, and ambiguous presentation of expiration dates on labels, contributed to a number of errors. Also, as part of the restocking process, EMS providers may discard bulky packaging and outer cartons that may contain critical information about the medication or help differentiate it from another look-alike product. Additionally, the cramped, often poorly lit environment of an EMS vehicle or aircraft (lighting must be low for an aircraft pilot to see at night) and the pressures inherent in emergency situations, further contribute to the risk of product selection errors.2
Example: During a resuscitation attempt on scene, a paramedic mistakenly selected and injected morphine instead of EPINEPHrine due to similar vial sizes and look-alike labels and cap colors.
Opportunities for Improvement: For purposes of stocking an EMS vehicle or aircraft, it is important to choose products, if possible, that do not look alike and have easy-to-read labeling and packaging (e.g., prefilled, clearly labeled, ready-to-administer syringes instead of vials with hard-to-read labels). Store all EMS medications and solutions with the principal display panel of the label facing forward to better enable reading, rather than in a top-up presentation in which only the cap is visible. Conduct a failure mode and effects analysis (FMEA) before removing drug containers from cartons to ensure all critical information is clearly evident on the immediate container label and that the product does not look similar to another stored in the same location. Encourage EMS providers to report look-alike containers to their distribution pharmacy so they can be purchased from different manufacturers to better distinguish them. The pharmacy that supplies EMS medications and solutions can assist by applying auxiliary labels to products with similar or ambiguous drug names, packaging, or labeling.
Subtheme 2: Erroneous IV Mixing, Dosing, and Administration
Challenges: To administer IV medications, EMS providers may need to carry out several related tasks, such as inserting a venous catheter, calculating drug doses, preparing admixtures, setting up and programming an infusion pump, and/or connecting the delivery device to the correct access port. The analysis of event reports identified several factors contributing to the risk of error when performing these tasks, including the use of complex dosing regimens, the need for EMS providers to mix IV infusions, complicated pump adjustments for different medication concentrations and flow rates, inaccessible protocols, and the lack of adequate and visible labeling to identify different patient access lines. The failure to standardize concentrations was also a common contributing factor. In fact, each EMS crew may mix different concentrations of solutions based on where they are transporting the patient, as hospitals may use different standard concentrations, making it difficult to standardize to a single concentration, even within a specific EMS group.
Mixing Example: EMS providers gave a bolus of tranexamic acid 1 g in 100 mL over 10 minutes. Then, the crew mixed 1 g of tranexamic acid in 1,000 mL and programmed the infusion to run over 1 hour; this second preparation should have been 1 g of tranexamic acid mixed in 100 mL and administered over 8 hours. The crew noticed the mistake about 10 minutes after starting the infusion while affixing a preprinted label to the infusion bag.
Dosing Example: EMS providers gave a four-fold overdose of IV ondansetron to a pediatric patient weighing 11 kg, administering 4 mg instead of 1 mg. The EMS protocol allowed for up to 0.1 mg/kg of ondansetron for pediatric patients weighing less than 20 kg. The dosing protocol was inaccessible during transport, and the crew, relying on memory, mistakenly remembered the dosing protocol (4 mg) for pediatric patients weighing between 20 and 40 kg.
Administration Example: A medication intended for IV administration was inadvertently administered into the patient’s arterial line. Fortunately, the patient experienced no harm. The arterial line was later labeled to help distinguish it from the IV line.
Opportunities for Improvement: Whenever possible, standardize the concentrations of common EMS IV medications for adult and pediatric patients. To improve transitions in care and reduce the risk of errors, some healthcare providers are utilizing the concentrations found in Standardize 4 Safety, the first national, interprofessional effort to standardize medication concentrations. Require EMS providers to use smart infusion pumps (rather than buretrols) with dose error-reduction systems employed. Include these standard concentrations in pump drug libraries and make it easy for EMS providers to engage the drug library when programming infusion pumps.
As space permits, use commercially available premixed solutions (e.g., tranexamic acid 1 g in 100 mL) and prefilled syringes to reduce the risk of admixture or dosing errors (and contamination) (see Theme 4). When weight-based dosing (e.g., for pediatric patients) or a nonstandard concentration is required, provide dosing aids (e.g., Broselow tape, infusion rate calculator, dose calculation app,4 drug dosing cards, other tools that provide pre-calculated weight-based dosing5) to assist with or avoid complex calculations. Also, provide standardized dosage/infusion rate tables. Increase opportunities for EMS providers to practice and perform pediatric weight-based dosing using scenario-based simulation training.5 Ensure key dosing and treatment protocols are readily accessible (e.g., online, on mobile devices, printed copies) to EMS providers so they do not have to rely on memory. Provide crews with labels for different access lines and encourage their use.
Subtheme 3: Gaps in Medication- and Equipment-Related Knowledge
Challenges: EMS providers, particularly paramedics, are trained to use a variety of medications, medical devices, equipment, and supplies to care for patients. However, it can be challenging for them to become knowledgeable about all of the various medications and equipment they may use. For example, previous studies have found that EMS providers may overuse sedation in patients with head injuries.2 In addition, our analysis found some errors were associated with unfamiliarity with EMS equipment or the patient’s own medical equipment or device, which was infrequently encountered.
Example: A paramedic mistakenly connected a patient’s oxygen tube to the air outlet instead of the oxygen tank, which resulted in a dangerous reduction in the patient’s oxygen saturation. The paramedic thought the air outlet was an oxygen outlet.
Opportunities for Improvement: All medications, devices, equipment, and situations encountered by EMS personnel cannot be anticipated. Nonetheless, during initial and ongoing EMS provider training, simulations and debriefings should be used to familiarize providers with the most common medications administered, medical equipment available on EMS vehicles or aircrafts (e.g., defibrillators), and patient devices (e.g., insulin pumps) they may encounter.
Theme 3: Medication Errors Related to Communication during Transitions of Care
Challenges: Numerous reports highlighted medication errors resulting from incomplete or inaccurate care transitions between EMS providers and other healthcare practitioners. EMS providers’ work can be complicated by communicating among each other amidst a noisy and hectic environment or via headsets or radio when in an emergency vehicle or aircraft. Errors or omissions during urgent or emergent patient handoffs with the final transfer facility (e.g., hospital) staff are frequent and understandable. Furthermore, although verbal information about the patient’s status is routinely shared during care transition, a complete written (or electronic) account of EMS care is often delayed. Any delay in documentation and interim absence of information can affect patient care.
Example: An EMS patient was brought to a hospital by ambulance. During a verbal hand-off to hospital providers, the EMS crew said that the patient had no allergies. In the hospital, a penicillin-related antibiotic was administered to the patient. Later, when the EMS crew provided the hospital with documentation of prehospital care, the hospital staff read that the patient was allergic to penicillin. Fortunately, the patient did not experience an adverse reaction to the antibiotic.
Opportunities for Improvement: While immediate transcription of information communicated between EMS providers and transfer facility staff is not always feasible, repeating back important communications can help verify understanding of critical information in a chaotic and noisy environment. However, immediate transcription and read-back of all verbal medication orders from an emergency command center is paramount. A standardized checklist to use for verbal hand-offs at the conclusion of transport, which includes the need for timely written documentation, may be helpful to avoid inaccuracies or omissions of essential patient information.
Theme 4: Medication Errors Related to Inventory Management
Challenges: Space restrictions in EMS vehicles and aircraft have led to crowded medication storage and the inability to separate look-alike medication packages and/or segregate certain high-alert medications (e.g., neuromuscular blocking agents). Additionally, space limitations have led some EMS crews to stock medication vials rather than larger, ready-to-use prefilled syringes for emergency medications (e.g., EPINEPHrine, sodium bicarbonate, atropine). During our analysis, several errors were associated with the lack of standardizing the contents and placement of medications in EMS drug bags, boxes, backpacks, or storage pockets. Several incidents involved finding previously prepared syringes, partially used single-dose vials, or expired medications in EMS supplies.
Example: EMS providers discovered a syringe containing morphine in a medical kit. The syringe had been prepared during a previous call but was never used.
Opportunities for Improvement: EMS medication storage design should include human factors considerations, including the importance of placing each piece of equipment and every medication in its correct location, organizing medications so they are easily retrievable, and preventing needlestick injuries, inadvertent exposure to medications, drug diversion, and delays in administering critical care medications. Provide prefilled syringes and commercially available premixed solutions whenever possible—the safety gains and immediate access to ready-to-use critical care medications and infusions are well worth the additional space that might be required for storage. Avoid stocking multiple concentrations of a particular medication.5 Regular review of the inventory maintained within the EMS vehicle or aircraft, as well as timely and appropriate restocking of medical supplies and medications, is essential. Checking specialty (e.g., pediatric) equipment and medications daily using a checklist may be helpful. In addition, routine checks of existing stock in EMS vehicles for expired/partially used medications and smart inventory monitoring systems that detect out-of-date and low-volume stock and automatically reorder it, ensures providers will have life-saving medications on-hand.
ISMP thanks ISMP Canada for sharing its recent analysis of paramedicine events, the themes and subthemes uncovered, and recommendations for improvement.3 ISMP also thanks GregORY P. Burger, PharmD, CPPS, FASHP, EMT, for his assistance with identifying areas of medication risk and improvement opportunities in paramedicine.
References
- Choi BY, Blumberg C, Williams K. Mobile integrated health care and community paramedicine: an emerging emergency medical services concept. Ann Emerg Med. 2016;67(3):361-6.
- Bigham BL, Morrison LJ, Maher J, et al. Patient safety in emergency medical services. Advancing and aligning the culture of patient safety in EMS. Edmonton (AB): Canadian Patient Safety Institute. Posted August 30, 2018.
- ISMP Canada. Multi-incident analysis of incidents involving paramedicine. ISMP Canada Safety Bulletin. 2020;20(1):1-4.
- Baumann D, Dibbern N, Sehner S, Zöllner C, Reip W, Kubitz JC. Validation of a mobile app for reducing errors of administration of medications in an emergency. J Clin Monit Comput. 2019;33(3):531-9.
- Cicero MX, Adelgais K, Hoyle JD, et al. Medication dosing safety for pediatric patients: recognizing gaps, safety threats, and best practices in the emergency medical services setting. A position statement and resource document from NAEMSP. Prehosp Emerg Care. August 2020;1-13.
Access this Free Resource
You must be logged in to view and download this document.