
We recently learned about three cases of accidental spinal injection of tranexamic acid instead of a local anesthetic intended for regional (spinal) anesthesia. Container mix-ups were involved in each case. In one case, a patient scheduled for knee surgery received tranexamic acid instead of bupivacaine. The anesthesiologist immediately realized the error, but by then, the patient began to experience seizures. The patient later recovered. In a second case, a patient undergoing hip replacement surgery received tranexamic acid instead of a local anesthetic for spinal anesthesia. The patient survived but also experienced seizures and had extreme pain due to arachnoiditis. In a third case, a patient scheduled for bilateral knee replacement also inadvertently received tranexamic acid instead of bupivacaine for spinal anesthesia. The patient experienced seizures, which necessitated placing her into an induced coma for several days.
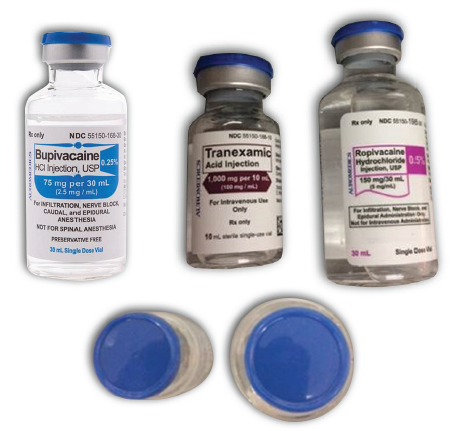
We previously reviewed errors with tranexamic acid in our May 23, 2019, ISMP Medication Safety Alert!. We noted that in the US, bupivacaine, ropivacaine, and tranexamic acid are packaged in vials that may have the same blue color cap (Figure 1). While label colors and vial sizes may be different, when the vials are stored upright near each other, only the blue caps may be visible, making it more difficult to differentiate one drug from the other. To make matters worse, these drugs are often found in areas where barcode scanning may not have been implemented or is not routinely utilized (e.g., perioperative areas, labor and delivery, emergency department). So, mix-ups are less likely to be detected. Unfortunately, the literature has additional reports of serious medication errors due to mix-ups between tranexamic acid and bupivacaine or ropivacaine during regional anesthesia. Syringe labeling issues may also contribute to such errors.
Tranexamic acid is an antifibrinolytic that prevents the breakdown of fibrin, thus promoting clotting. It is approved for short-term use (2-8 days) in patients with hemophilia to reduce the risk of hemorrhage during and following tooth extraction; however, it is also used off-label in a variety of hemorrhagic conditions to control bleeding, including postpartum hemorrhage. Although tranexamic acid is not indicated for joint surgeries, it is often used intravenously (IV) or topically during these procedures to decrease blood loss. Tranexamic acid is also available as an oral tablet for the treatment of cyclic heavy menstrual bleeding in women.
When given via the spinal route in error, tranexamic acid is a potent neurotoxin that is harmful to patients, with a mortality rate of about 50%. Survivors often experience seizures, permanent neurological injury, ventricular fibrillation, and paraplegia (Palanisamy A, Kinsella SM. Spinal tranexamic acid–a new killer in town. Anaesthesia. 2019;74[7]:831-3).
Prevention measures
-
Separate or sequester tranexamic acid in storage locations and avoid storing local anesthetics and tranexamic acid near one another.
-
To prevent reliance on identifying the drug by viewing only the vial caps, never store injectable drug vials in an upright position, especially when stored in a bin or drawer below eye level. Store them in a way that always makes their labels visible.
-
Minimize look-alike vials (caps) by purchasing these products from different manufacturers.
-
Consider purchasing labels that state, “Contains Tranexamic Acid” to place over the vial caps.
-
Utilize barcode scanning prior to dispensing as well as when accessing the drug in surgical and obstetrical areas.
-
Consider NRFit syringes and connectors for local anesthetics used for regional anesthesia administered via the neuraxial route. NRFit connectors are incompatible with Luer connectors, thus preventing misconnections with drugs intended for IV use, such as tranexamic acid (see ISMP’s July 16, 2020, article on NRFit).
-
Consider the use of pharmacy-prepared or commercially available premixed containers of tranexamic acid, which would be less likely to be confused with local anesthetic vials. Pharmacy preparation and labeling of syringes or infusions would help alleviate these errors. A premixed container of IV tranexamic acid in a sodium chloride solution for injection, 1 g/100 mL (10 mg/mL), is commercially available. While the only approved indication for tranexamic acid is to reduce or prevent hemorrhage for patients with hemophilia undergoing tooth extraction, this product could be used off-label to treat other forms of bleeding. However, vials of tranexamic acid may still be needed since loading doses may be required prior to infusion (or a smart infusion pump loading dose feature could be used that automatically switches to a continuous infusion once the loading dose has been delivered). Also note: local anesthetics may be available at some locations in premixed containers or prepared by pharmacy for use in regional anesthesia.
The National Alert Network (NAN) is a coalition of members of the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP). The network, in cooperation with the Institute for Safe Medication Practices (ISMP) and the American Society of Health-System Pharmacists (ASHP), distributes NAN alerts to warn healthcare providers of the risk for medication errors that have caused or may cause serious harm or death. NCC MERP, ISMP, and ASHP encourage the sharing and reporting of medication errors both nationally and locally, so that lessons learned can be used to increase the safety of the medication-use system.