
Confusion abounds! 2-year summary of the ISMP National Vaccine Errors Reporting Program (Part I)
According to the World Health Organization (WHO), immunizations prevent between 2 and 3 million deaths per year. Despite this success, many children and adults in the US remain vulnerable to the 17 vaccine-preventable diseases. Some people are vulnerable because they have not been offered vaccinations; others opt-out of recommended immunizations based in large part on misinformation. However, errors with vaccines can also result in unintended and unrecognized vulnerability, leaving patients unprotected against serious diseases such as hepatitis A, hepatitis B, diphtheria, tetanus, measles, cervical cancer, and many others.
In September 2012, ISMP (in cooperation with the California Department of Public Health) established the ISMP National Vaccine Errors Reporting Program (ISMP VERP) to collect data about the types of errors occurring and their underlying causes. In our November 28, 2013 newsletter, we provided a summary analysis of error reports submitted during its inaugural year. In this issue, we provide a 2-year summary of error reports submitted through October 2014.
Volume, types, and sources of reports
Between September 2012 and October 2014, a total of 884 reports were submitted to the ISMP VERP. The error reports provide a steady stream of information to ISMP for analysis so that prevention strategies can be identified and shared. In the past 2 years, reports have increased from 373 in 2013 to 425 so far in 2014 (January-October).
Most reports (89%) involved vaccine errors that reached patients. Those involving close calls (8%) or hazardous conditions (3%) were often associated with labeling and packaging concerns. An example of a reported hazard is the labeling of RABAVERT (rabies vaccine), which fails to draw attention to the required diluent and vaccine vials. The hazard may have led to administration of RabAvert diluent alone without the vaccine component.
The vast majority of vaccine error reports were submitted by practitioners who work in outpatient settings (Table 1) 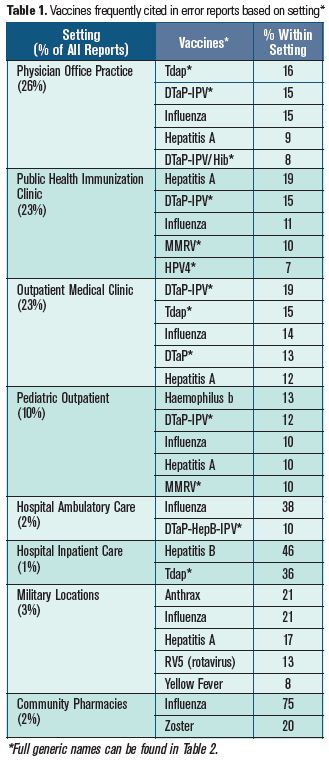 where most children and adults receive vaccines. Given its voluminous use, influenza virus vaccine errors were among the most frequently reported, accounting for 16% of all reports. However, errors related to other vaccines were more common in specific settings based on the typical populations served. For example, errors with the hepatitis A (HepA) and human papillomavirus (types 6, 11, 16, 18) (HPV4) vaccines were most commonly reported by staff in public health immunization clinics, and errors with the anthrax vaccine were most commonly reported by staff at military locations.
where most children and adults receive vaccines. Given its voluminous use, influenza virus vaccine errors were among the most frequently reported, accounting for 16% of all reports. However, errors related to other vaccines were more common in specific settings based on the typical populations served. For example, errors with the hepatitis A (HepA) and human papillomavirus (types 6, 11, 16, 18) (HPV4) vaccines were most commonly reported by staff in public health immunization clinics, and errors with the anthrax vaccine were most commonly reported by staff at military locations.
Medical assistants (27%), registered nurses (23%), and licensed practical nurses (11%) were most frequently involved in the reported errors. Physicians (8%), nurse practitioners (5%), and pharmacists (2%) were involved less frequently, suggesting that most of the reported errors are related to vaccine administration and not prescribing or dispensing. Medical assistants were most often involved in events that occurred in medical clinics, physician offices, or hospital ambulatory care facilities. Registered nurses were most often involved in events that occurred in public health clinics and pediatric facilities. These statistics may reflect the groups most likely to administer vaccines in these locations.
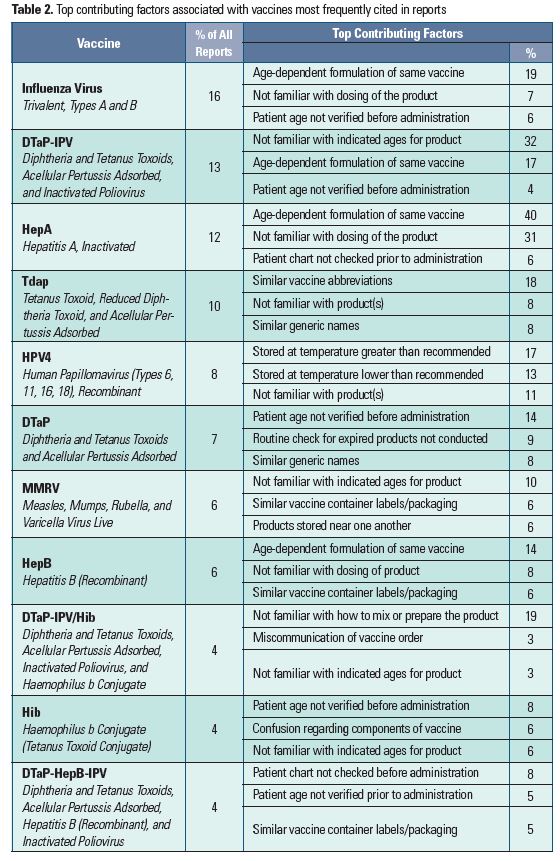
The most frequently reported vaccine errors can be found in Table 2, along with the most prevalent contributing factors for each vaccine. The Table also lists the full generic names of vaccines abbreviated in this report as established by the Advisory Committee on Immunization Practices (ACIP). Among all vaccine errors, age-related contributing factors were reported most often.
Influenza Virus Vaccine
The influenza vaccine is available in various formulations that differ based on patient age:
≥ 6 months FLUZONE, FLUZONE QUADRIVALENT
≥ 3 years FLUARIX, FLUARIX QUADRIVALENT, FLULAVAL, FLULAVAL QUADRIVALENT
≥ 4 years FLUVIRIN
≥ 9 years AFLURIA*
≥ 18 years FLUCELVAX, FLUBLOK
2 - 49 years FLUMIST QUADRIVALENT
18 - 64 years FLUZONE INTRADERMAL
≥ 65 years FLUZONE HIGH-DOSE
*Package insert says ≥ 5 years, but ACIP discourages use in children less than 9 years due to risk of febrile reactions.
Thus, it is not surprising that the most common type of influenza vaccine error reported to the ISMP VERP was related to administration of a vaccine to a patient who was not within the indicated age range for that vaccine. Most often, these errors were caused by a lack of knowledge regarding the age-dependent formulations or a failure to verify the patient’s age before administration to ensure the correct formulation was being administered. Also, the dosing (both regimen and volume) of various influenza vaccines differs in adults and children, which has led to dosing errors.
Some influenza vaccine errors were associated with mix-ups between vaccines with similar brand names or look-alike vaccine container labels or packaging, particularly when products accidentally found their way into the wrong bin or storage area or were kept in crowded storage areas. The vaccine has also been confused with other drugs. For example, in multiple cases, school nurses administering influenza vaccines to teachers accidentally prepared and administered insulin. A few errors were also associated with the administration of expired vaccines, and confusion regarding the correct route of administration or the correct administration technique. For example, two recently reported events during this influenza season dealt with administration of influenza vaccines to body sites that did not contain enough muscle—too high on the shoulder in one case, and too far back in the fatty tissue of the arm near the armpit in the other case. Both injections led to prolonged pain and significant adverse local reactions. We have also received numerous reports of administration of the intramuscular vaccine via the intranasal route.
DTaP (DAPTACEL, INFANRIX), Tdap (ADACEL, BOOSTRIX), DTaP-IPV (KINRIX), DTaP-HepB-IPV (PEDIARIX), or DTaP-IPV/Hib (PENTACEL) vaccines
The dominant issues reported with these vaccines are the same issues that have long been reported to ISMP and the US Food and Drug Administration (FDA)—confusion between the different age-dependent formulations and combination products that have led to administration of the wrong vaccine. For example, more than 50 errors have been reported in which DTaP (diptheria and tetanus toxoids, acellular pertussis) was administered instead of Tdap (tetanus toxoid, reduced diptheria toxoid, acellular pertussis), or vice versa. Tdap is for older children and adults as a booster dose, and DTaP is intended for children between 6 weeks and 6 years of age for initial immunization. Reports also suggest that Tdap has been mistakenly administered instead of Td (tetanus, diphtheria). In some previously reported cases, hundreds of patients have been involved in a single mix-up.
Several reports suggest that packaging similarities have also led to mix-ups between Kinrix and Pediarix, and Tdap and Pediarix. Similar or identical cap colors on vials have led to Kinrix administration instead of HPV (human papillomavirus vaccine). Hepatitis B (recombinant) (HepB) vaccine has been mistaken as Adacel given similar orange coloring on the vials. Vaccine vials placed in the wrong bin in automated dispensing cabinets have also led to unintended vaccinations.
We have received dozens of reports of patients given a combination vaccine when only one component was needed or when components in the administered vaccine differed from those that were intended. For example, numerous reports involved administration of Kinrix by staff who mistakenly thought it contained HepB, and misadministration of Pediarix, believing it contained Hib (Haemophilus influenzae type b conjugate), not IPV (inactivated poliovirus). Complex vaccination schedules have contributed to mistakes with the timing of these vaccines, particularly when children are following an alternate or delayed schedule of immunizations. We have also received numerous reports of children 7 years and older receiving Pediarix (DTaP-HepB-IPV), which is intended for younger children (i.e., at 2, 4, and 6 months of age).
Another problem detailed in numerous reports involved administration of a single vaccine already contained in a combination vaccine given at the same time. For example, one patient received Pentacel along with separate DTaP and IPV vaccinations, thus receiving duplicate DTaP and IPV along with the Hib component in Pentacel. Giving just one component instead of the intended combination vaccine has also been reported. Confusion has led to administration of both Pediarix and HepB instead of the intended Hib, which can sound or look like “HepB.” Thus, extra doses have been an ongoing problem with the combination vaccines.
Errors reported with Pentacel continue to include administration of just one of the two required vials of product. One vial contains DTaP-IPV liquid and the other contains Hib powder. An event reported recently involved a nurse who reconstituted Hib powder using sterile water instead of using the DTaP-IPV liquid included in the Pentacel carton.
One thing is clear—2 years of data in the ISMP VERP confirms that confusion abounds given the plethora of incorrect abbreviations used for this group of vaccines and erroneous statements in the narrative reports regarding the actual components of combination vaccines, dosing schedules, and intended ages.
Hepatitis A (HAVRIX, VAQTA) or hepatitis B (ENGERIX-B, RECOMBIVAX HB) vaccines
The most frequent errors reported with HepA and HepB vaccines involved dosing errors in which a child received an adult’s dose or an adult received a child’s dose, mix-ups between the two vaccines, and timing errors in which the vaccines were given at the wrong age or interval—usually too soon after the first dose. This year, there were also numerous reports of patients receiving an extra dose of the vaccine due to inaccuracies in state immunization registries or duplicate orders entered into an electronic record. Even when immunization records were accurate, doses given at too-short intervals were reported without a clear explanation regarding why it happened.
Specific to HepB, several reports indicated that an infant had received the first vaccine dose at birth while in the hospital, but the physician’s office staff was unaware of this information and administered an extra dose in the series to a child during the first year. The reports imply that the parents were responsible for reporting the birth dose to the physician’s office and had failed to do so. A worse problem is when the vaccine is not given at birth (within the first 12 hours of life) prior to hospital discharge, and may be missed entirely.
Repeated mix-ups have been reported between the two vaccines and others, specifically Hib, the influenza vaccine, and HPV4. Close proximity of vaccines in refrigerators was often cited as a factor. In one report, a nurse reached into the refrigerator to obtain a HepB vaccine, but she accidentally pulled out a vial of HepA vaccine, which was sitting right beside it. The nurse read the label but only verified “hepatitis” and subsequently gave the dose to the child. Numerous reports have also been received regarding the administration of both Engerix-B and Pediarix, which both include a hepatitis B component.
Human papillomavirus vaccine (HPV4) (GARDASIL)
Most of the errors reported with HPV4 were due to temperature extremes in which the vaccine was exposed to temperatures greater than or less than recommended. In one case, three vials that had been exposed to excessive temperatures for an extended period of time were gathered to be returned to the pharmacy provider. However, these three vials were inadvertently used to immunize patients at a pediatric health facility, as they were not labeled as unusable or sequestered away from other medication supplies. A few errors occurred when the vaccine was administered to children younger than 9 years of age or when the vaccine was given unnecessarily beyond the recommended series. Mix-ups have also been reported between HPV4 and other vaccines, including human papillomavirus (types 16, 18) (HPV2), which was administered to male patients by staff who believed it was HPV4. Mix-ups with HepB, IPV, and PNEUMOVAX 23 (pneumococcal polysaccharide) (PPSV23) vaccines have also been reported.
Measles, mumps, rubella, and varicella vaccine (MMRV) (PROQUAD)
The MMRV vaccine has been erroneously administered via the intramuscular route rather than the subcutaneous route. A few errors involved vaccine administration to an infant less than 12 months or children older than 12 years. Mix-ups in the schedule of doses have also been reported, particularly when international travel was anticipated. Recently, numerous reports note that patients received ProQuad and a varicella vaccine at the same time. Several of these reports reveal that staff members administering the vaccines did not know that varicella was a component of ProQuad. Other reports indicate that only “MMR” was seen when quickly viewed on the ProQuad box label, so the product was thought to contain only measles, mumps, and rubella vaccine. ProQuad has also been given in error when only MMR has been prescribed. In September 2014, 15 children died in Syria after the diluent used to reconstitute a measles vaccine turned out to be atracurium, a neuromuscular-blocking agent. Given that ProQuad is supplied in single-dose vials of lyophilized vaccine along with vials of sterile water diluent, reconstitution with the wrong diluent is likewise possible with the MMRV vaccine.
Wrong patient errors
Unrelated to a specific type of vaccine, we continue to receive multiple reports of vaccines administered to the wrong child when more than one child was present in the exam room or medication administration area. Several of the reports describe the confusion that ensues when several children are crying and a parent is trying to calm them down. Parents often bring siblings into the office for immunizations together, raising the risk of giving one child a vaccine intended for another child. To cite an example, an infant was supposed to receive DTaP and his toddler sister was to receive a HepA vaccine. But the infant received the HepA vaccine before the mix-up was discovered. In this case, the mother of the children reported the error, thus additional information was not provided. In another case, ProQuad intended for a young boy was given to his 13-year-old sibling.
Wrong diluent errors
While several examples of using the wrong diluent to prepare vaccines were reviewed above, errors of this type were reported frequently for several other vaccines. There are currently 12 vaccines that have specific diluents, and 2 vaccines that have two-component containers that must be mixed prior to administering the dose. Typically, the practitioner dispensed or administered just the manufacturer-supplied diluent, or the practitioner reconstituted a lyophilized vaccine using an unintended diluent instead of the specific diluent provided. These errors were reported most frequently with the Hib vaccine, which comes with a vial of 0.4% sodium chloride, provided by the manufacturer, to be used as a diluent. Reported errors with these vaccines frequently involve multiple patients. In other cases, a practitioner dispensing or administering the vaccine failed to notice that a single dose requires combining the contents of two vials. Many times, these vials look very similar and both may emphasize the name of the active drug. Several errors also suggest that practitioners may mistakenly believe the “liquid” component of the vaccine is just a standard diluent. These errors were reported most frequently with MENVEO (meningococcal [groups A, C, Y, and W-135] diphtheria conjugate) and Pentacel.
Conclusion
The ISMP VERP 2-year summary provides new details regarding how vaccine errors happen, which we will continue to use as we hone in on vaccine safety. Early in 2015, we plan to publish a follow-up article (Part II) recapping the main risks and offering recommendations to reduce the risk of vaccine errors. We extend our sincere thanks to those who have submitted reports to the ISMP VERP, and we encourage all of our readers to join in these efforts.