
First Annual Review of Data Submitted to the ISMP National Vaccine Errors Reporting Program (ISMP VERP)
According to the Centers for Disease Control and Prevention (CDC), 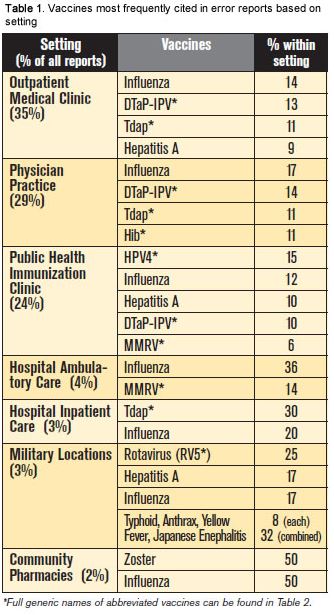 immunizations are one of the greatest success stories in public health, helping to eradicate some serious illnesses such as smallpox from the globe and reducing many infectious diseases to an all-time low. However, if errors happen when prescribing, dispensing, or administering vaccines, the adverse impact on disease prevention could be significant, particularly to individuals who are not fully protected or have experienced a preventable adverse vaccine event. In September 2012, ISMP partnered with the California Department of Public Health to develop the ISMP National Vaccine Errors Reporting Program (ISMP VERP) to promote ongoing learning about potentially preventable harm associated with adult and pediatric immunizations. After collecting reports from across the nation for over a year, ISMP provides an overview of what has been learned about vaccine safety from the reports submitted to the program.
immunizations are one of the greatest success stories in public health, helping to eradicate some serious illnesses such as smallpox from the globe and reducing many infectious diseases to an all-time low. However, if errors happen when prescribing, dispensing, or administering vaccines, the adverse impact on disease prevention could be significant, particularly to individuals who are not fully protected or have experienced a preventable adverse vaccine event. In September 2012, ISMP partnered with the California Department of Public Health to develop the ISMP National Vaccine Errors Reporting Program (ISMP VERP) to promote ongoing learning about potentially preventable harm associated with adult and pediatric immunizations. After collecting reports from across the nation for over a year, ISMP provides an overview of what has been learned about vaccine safety from the reports submitted to the program.
Source, volume, and types of reports
From September 2012 through October 2013, a total of 433 reports were submitted to the ISMP VERP. Most reports (90%) involved vaccine errors that reached patients. The remaining reports were classified as close calls (6%) (errors that happened but did not reach the patient) or hazardous conditions that warrant concern (4%). The vast majority of reports were submitted by practitioners who work in outpatient settings, where most children and adults receive their vaccines (Table 1). As expected, given its widespread use annually, errors with the influenza virus vaccine were among the most frequently reported. However, errors related to other vaccines were more common in specific settings based on the typical populations served. For example, errors with the zoster vaccine were most commonly reported by staff in community pharmacies.
Medical assistants (38%) and registered nurses (37%) were most frequently involved in the reported errors or hazardous conditions. Medical assistants were most often involved in events that occurred in outpatient settings such as medical clinics, physician practices, or hospital ambulatory care centers. Registered nurses were most often involved in events that occurred in public health clinics. These statistics may reflect the groups that are most likely to administer vaccines. Licensed practical nurses (15%), physicians (5%), pharmacists (2%), and other healthcare practitioners (3%) were involved in fewer events.
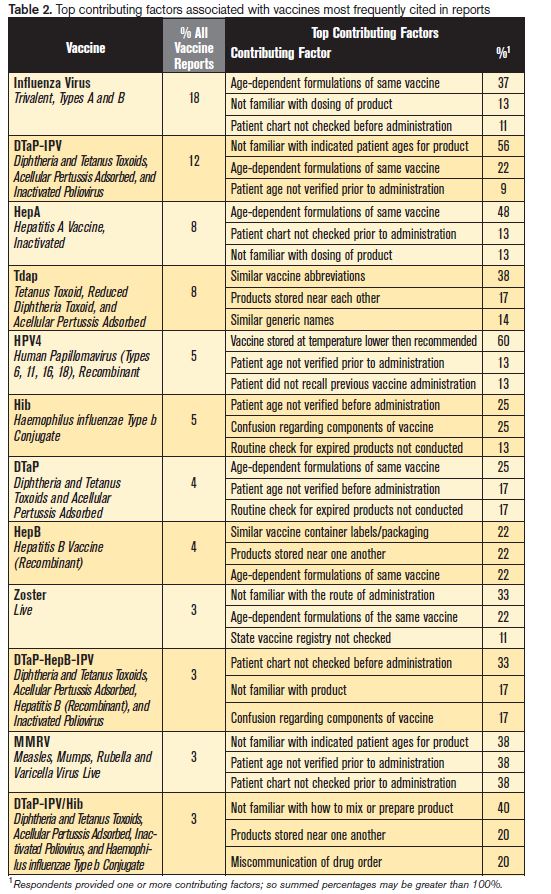
The most common vaccine errors reported can be found in Table 2, along with the most prevalent contributing factors. Table 2 also lists the full generic names of vaccines abbreviated in this report using standard abbreviations established by the Advisory Committee on Immunization Practices (ACIP). Among all vaccine errors, age-related contributing factors were reported most often (40%), specifically:
- Confusion between numerous age-dependent formulations that target the same infections (18%)
- Unfamiliarity with dosing and timing of vaccines based on the patient’s age (14%)
- Failure to verify the patient’s age prior to administration (8%)
Common contributing factors were identified for each vaccine listed in Table 2.
Influenza vaccine
The influenza vaccine is available in multiple formulations that differ in their labeled indications for age:
- > 6 months (FLUZONE, FLUZONE QUADRIVALENT)
- > 3 years (FLUARIX, FLUARIX QUADRIVALENT, FLULAVAL, FLULAVAL QUADRIVALENT)
- > 4 years (FLUVIRIN)
- > 9 years (AFLURIA)
- > 18 years (FLUCELVAX)
- > 18-49 years (FLUBLOK)
- Adults ≤ 49 years (FLUMIST, FLUMIST QUADRIVALENT)
- 18-64 years (FLUZONE INTRADERMAL)
- > 65 years (FLUZONE HIGH-DOSE)
Thus, it is not surprising that the most common type of influenza vaccine error reported to the ISMP VERP is associated with administration of one form of the vaccine to patients who are not within the indicated age range. Furthermore, the dosing of various influenza vaccines differs for adults and children, leading to errors in which a young child has received an adult’s dose and an adult has received a young child’s dose. Most often, these errors were caused by a lack of knowledge about the different age-dependent formulations. Occasionally, the error was caused by a mistaken assumption of the patient’s age that was unconfirmed. Extra vaccine doses or administration of a second dose (when indicated) too soon were also reported due to erroneous documentation on the record or a failure to check the medical and/or vaccine record prior to administration.
Influenza vaccine errors were also associated with the wrong route of administration or technique errors. For example, a pharmacist administered the vaccine to a coworker high above the deltoid muscle, which led to tendon damage requiring steroid injections and physical therapy. In another case, a nurse injected a needle into the patient’s deltoid muscle but then noticed that the syringe was empty. She took the needle out, disposed of it, and prepared a new dose of the influenza vaccine. Several hours later, the nurse wondered if the empty syringe had been used for a previous patient. Another report described an error in which 25 patients had been given an intramuscular formulation of the influenza vaccine via the intranasal route, which required revaccination. Other reports suggest that the intramuscular influenza vaccine has been given subcutaneously.
Numerous error reports were associated with giving the influenza vaccine by mistake instead of some other intended vaccine. For example, a dose of Fluarix (influenza vaccine) had been misplaced in a box of TWINRIX (hepatitis A [inactivated] and hepatitis B [recombinant] vaccine), and the practitioner did not notice until after the influenza vaccine had been given. In another case, a patient received PEDIARIX (DTaP-HepB-IPV) instead of the influenza vaccine.
A hazard report not associated with an error described a concern regarding the labeling of Sanofi Pasteur’s Fluzone High-Dose syringes. The text on the barrel is black on a dark gray background, and the plunger is black, making it difficult to read the label information. The reporter suggests making the background white, as with the expiration date and lot number, which can be seen clearly (image unavailable).
DTaP (DAPTACEL, INFANRIX), Tdap (ADACEL, BOOSTRIX), DTaP-IPV (KINRIX), DTaP-HepB-IPV (PEDIARIX), or DTaP-IPV/Hib (PENTACEL) vaccines
The dominant issues reported with these vaccines are the same issues that have long been reported to ISMP and FDA—confusion between the different age-dependent formulations and combination products. For example, repeated errors have been reported in which DTaP was administered instead of Tdap, or vice versa. Tdap is intended for older children and adults as a booster, and DTaP is intended for children between 6 weeks and 6 years of age for initial immunization. We have also received numerous reports of children 7 years and older receiving Pediarix (DTaP-HepB-IPV), which is intended for younger children. Complex vaccination schedules have contributed to mistakes with the timing of these vaccines, particularly when children are following an alternate or delayed schedule of immunizations.
Numerous reports suggest that name and packaging similarities with Kinrix and Pediarix have led to mix-ups. One reporter also noted that Kinrix should be labeled more clearly regarding its approved use only in children 4-6 years old—many reports note that the vaccine has been given to children younger and older than the appropriate age range. In one case, the mother of a 2-month-old child was very nervous about vaccinations and initially wanted her child to only receive DTaP. She later changed her mind, so the nurse discarded the DTaP and inadvertently gave the infant Kinrix since it was a combination product, forgetting that it is intended for children 4-6 years old.
Combination vaccines have also been given along with individual doses of their component vaccines. For example, numerous reports have been received regarding the administration of both Pediarix along with DTaP or hepatitis B vaccine (both components of Pediarix). The opposite error—giving just one component instead of the intended combination vaccine—has also been reported. Confusion has also led to administration of both Pediarix and hepatitis B (HepB) instead of the intended Hib (Haemophilus influenzae type b conjugate), which sounds like “HepB.” Extra doses have also been a problem with the combination vaccines. In one error report, a child who needed his fourth dose of DTaP was given Pediarix, thus receiving an unnecessary dose of hepatitis B and IPV. There are also multiple reports of just the sterile diluent being administered without the associated vaccine that should have been reconstituted with the diluent.
The variety of combination products and their indication for specific doses in a vaccine series also increases the risk of errors. For example, Pentacel can be used to complete the first 4 doses of the DTaP or IPV series but it should not be used for the polio booster dose given at 4-6 years of age; Kinrix should be used.
Besides mix-ups within these various DTaP-related vaccine products, we have also received reports regarding administration of a totally different vaccine product in error. For example, Kinrix was administered instead of GARDASIL (human papillomavirus vaccine)—both vials had green colored tops. Hepatitis B (recombinant) vaccine (ENGERIX-B) was administered instead of Tdap (Adacel)—both had orange caps and orange markings on the label, and the Engerix-B vial was found in a refrigerator bin reserved for Adacel. In another case, two infants received Tdap instead of the intended hepatitis B vaccine. In this case, the hepatitis B vaccine was selected from an automated dispensing cabinet and retrieved from a refrigerator also stocked with vaccines for mothers.
Errors reported with Pentacel were almost exclusively due to administration of just one of the two required vials of product. One vial contains DTaP-IPV liquid and the other contains Hib powder. Almost all reported errors were associated with administering just the DTaP-IPV component, or reconstituting the Hib powder with a sterile diluent and administering it alone.
Hepatitis A (HAVRIX, VAQTA) or hepatitis B (ENGERIX-B, RECOMBIVAX HB) vaccines
The most frequent errors reported with hepatitis A vaccine or hepatitis B vaccine involved dosing errors in which a child received an adult’s dose and an adult received a child’s dose, as well as timing errors in which the vaccines were given at the wrong age or interval—usually too soon after the first dose. Mix-ups between the two vaccines and others, specifically Hib, have also been reported. In one case, a telephone order for Hib was misheard by a pharmacist who dispensed hepatitis B vaccine in error, and the patient was given the wrong vaccine. Numerous reports have been received regarding the administration of both Engerix-B and Pediarix, which includes a hepatitis B component.
Human papillomavirus vaccine (HPV4) (GARDASIL)
Most of the errors reported with Gardasil were due to temperature excursions in which the vaccine was exposed to temperatures below 36 degrees Fahrenheit. A few errors occurred when the vaccine was administered to children younger than 9 years of age or unnecessarily beyond the recommended series of doses.
Haemophilus influenzae type b conjugate vaccines (ACTHIB, HIBERIX, PEDVAXHIB)
Most events reported with the Haemophilus influenzae type b conjugate vaccine involved errors in which the Hib vaccine was administered according to the wrong schedule. The administration schedule for PedvaxHIB typically calls for 3 doses, whereas the schedule for ActHIB typically requires 4 doses. One hospital reported that its electronic health record was set up for a 4-dose schedule, so errors were made when they began using PedvaxHIB.
Zoster vaccine (ZOSTAVAX)
Mix-ups between the zoster vaccine and the varicella vaccine (VARIVAX) were frequently reported, with children receiving the zoster vaccine and adults receiving the varicella vaccine in error. Extra doses of the zoster vaccine were also given in error because state vaccine registries were not checked. Several reports also noted that the zoster vaccine was given by the intramuscular route rather than the subcutaneous route of administration.
Measles, mumps, rubella, and varicella vaccine (MMRV) (PROQUAD)
As with the zoster vaccine, the MMRV vaccine has been erroneously given by the intramuscular route rather than the subcutaneous route of administration. A few errors involved vaccine administration to an infant less than 6 months old and mix-ups in the schedule of doses, particularly when international travel was anticipated.
General errors
Unrelated to a specific type of vaccine, we received multiple reports of vaccines administered to the wrong child when more than one child was present in the exam room or medication administration area. Several of the reports describe the confusion that ensues when several children are crying and a parent is trying to calm them down. Parents often bring siblings into the office for immunizations together, raising the risk of giving one child a vaccine intended for another child. In one report, a nurse and medical assistant prepared the vaccines for 2- and 4-year-old siblings in the same exam room. Distracted by the anxious children, staff accidentally picked up the wrong tray of syringes and administered the vaccines to the wrong children.
Conclusion
The ISMP VERP provides a rich new resource for learning about vaccine errors. This preliminary analysis of the reports to date offers just a hint of what’s to come in the future as we hone in on vaccine safety. While some of the errors in this new reporting system have been reported previously to the ISMP National Medication Errors Reporting Program (ISMP MERP), we are excited to be receiving additional reports from inpatient and outpatient healthcare providers, which will help to fill the gap of knowledge regarding this area of vaccine safety. In this analysis of the data, we have introduced new details regarding vaccine errors and how they are happening. Early in 2014, we plan to publish a follow-up article recapping the main risks and making recommendations to reduce the risk of vaccine errors. We extend our sincere thanks to those who have submitted reports to the ISMP VERP and we encourage all of our readers to continue these efforts.