
Unverified Patient-Reported Error: A False Alarm Can Have Real Consequences
When faced with a possible medication error, obviously, one should never assume that it is just a false alarm. Timely investigation is required, and a high index of suspicion is paramount. On the other hand, assuming that patient-reported events are always accurate can also be dangerous and costly if they are not verified via a timely investigation. In an unusual turn of events, we recently learned about a false alarm that set into motion unnecessary anxiety and wasted resources when a potentially fatal error was suspected, but not confirmed. The false alarm involved a patient who reported too-rapid home infusion of chemotherapy, but later analysis revealed that no error had actually occurred.
The patient-reported error
A cancer patient was receiving her second cycle of IV fluorouracil as a continuous infusion over 4 days via a Leventon Dosi-Fuser (Figure 1), a portable elastomeric delivery system. A hospital pharmacy had prepared the chemotherapy, but the patient was receiving the infusion at home, with delivery and follow-up by a home-infusion service. After 1 day, the patient called the home-infusion triage nurse to report that the entire contents of the infusion had been delivered over 30 hours instead of the planned 96 hours (4 days). The nurse called the covering oncology fellow, who recommended sending the patient to the emergency department (ED) for evaluation. 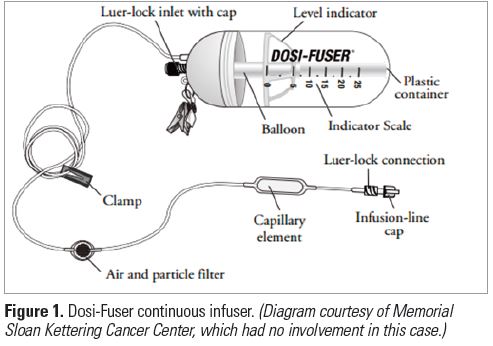
After advising the patient to go to the ED, the triage nurse called the ED charge nurse and physician to alert them to the impending visit for what appeared to be a fluorouracil overdose due to a delivery device failure. The home-infusion triage nurse also contacted the on-call home-infusion pharmacist, who then called her supervisor. The home-infusion service asked the nurse to save the device so it could be inspected the following day.
The patient presented to the ED and was evaluated by a nurse and physician (different than the nurse and physician initially contacted by the triage nurse). The nurse had received report from the charge nurse and believed the too-rapid infusion had been confirmed. She never saw a Leventon Dosi-Fuser before and, although she looked at it, she failed to notice that the solution had NOT entirely infused. Using personal protective equipment, she disconnected the Dosi-Fuser from the patient and placed it into a hazardous waste bag. The oncologist came to the ED and looked at the device through the bag. He also was not familiar with the device and assumed it was empty. He did not remove it from the bag for closer inspection because it contained chemotherapy and was labeled as hazardous waste.
Both the oncologist and the emergency department physician had called poison control and were told that the rapid infusion of fluorouracil could cause a potentially fatal overdose that should be treated accordingly. The oncologist made arrangements for the patient to receive an investigational antidote, uridine triacetate (formerly vistonuridine), which would require air freight delivery from a distant state. This was ordered with the assistance of the inpatient pharmacist, who also took possession of the Dosi-Fuser device. The inpatient pharmacist called his assistant director, who alerted their director, but no one from the inpatient pharmacy actually looked at the Dosi-Fuser device.
The next morning, word of the error reached the ambulatory oncology center pharmacist. He retrieved the device that was removed from the patient and immediately noticed that it did not “feel” empty—this was obvious to him and his staff because they handled the devices often. After closer inspection and weighing the device, they learned it was NOT empty, and no overdose had occurred. Fortunately, because the uridine triacetate had not yet arrived, the patient did not receive the antidote. The patient was reassured that she did not receive an overdose and was discharged home.
There are a number of lessons to be learned from this event, many of which can help avoid a false alarm or a failure to see and appreciate important risks.
Confirm patient-reported errors
Issue: The triage nurse trusted the patient’s self-report of a too-rapid infusion without further investigation. The patient sounded knowledgeable and had received a previous course of therapy, so the nurse thought the patient was fully credible. The patient was a nurse (unknown at the time of the event) and spoke in a manner in which others would trust what she was saying. Knowing nothing about the specific device, the triage nurse did not ask the patient to confirm that the level indicator was at zero. After contacting the on-call home-infusion pharmacist, the triage nurse made an (appropriate at the time) assessment that time was of the essence, so he sent the patient to the ED believing this represented a higher level of care that could better assess the potential error more effectively. However, the ED staff were not familiar with the device either.
Lesson learned: While reports of errors or other concerns from patients about medications should never be dismissed without a thorough investigation, neither should they be accepted without an assessment by staff with experience in the processes of care involved in the event, or the equipment or technology under evaluation. In this case, the ambulatory oncology center pharmacist or hospital pharmacy that filled the device should have been consulted. However, if timely treatment of a potential error is of the essence, err on the side of caution and begin the process of treatment while conducting a full investigation.
Keep a high index of suspicion
Issue: None of the healthcare professionals who encountered the patient considered scenarios outside of a device failure as a cause for the “error.” Other possibilities that should have been considered include: the device could have been filled with the wrong volume; the pharmacy could have used the wrong infuser type; or the patient was mistaken.
Lesson learned: Contact healthcare providers recently involved in the care of a patient and consider all reasonable scenarios when determining cause and effect.
Examine evidence during handoffs
Issue: There were multiple handoffs during the patient’s initial assessment and care: home-infusion triage nurse to ED charge nurse to ED staff nurse; ED physician to another ED physician; oncology fellow to oncologist; multiple pharmacists. During these handoffs, everybody assumed someone else had confirmed the overdose.
Lesson learned: When possible, practitioners should examine any evidence that is available during handoffs to be sure they understand and verify any patient care issues associated with a hazardous condition or potential/actual error.
Promote inspection and monitoring
Issue: Even if the home-infusion triage nurse had asked the patient to confirm placement of the level indicator (Figure 1), it was difficult to see because of the placement of 2 large labels on the container (Figure 2). 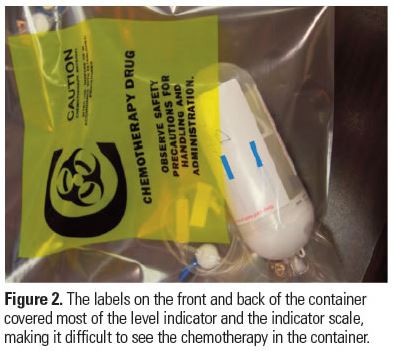 This likely contributed to the patient’s misunderstanding that the bottle was empty. The labels also inhibited the ability of the ED nurse, pharmacists, oncology fellow, and oncologist to visualize the indicator. While they could have visualized it by peeling back the label, this is not something they would be expected to do.
This likely contributed to the patient’s misunderstanding that the bottle was empty. The labels also inhibited the ability of the ED nurse, pharmacists, oncology fellow, and oncologist to visualize the indicator. While they could have visualized it by peeling back the label, this is not something they would be expected to do.
Lesson learned: Make sure that labels or other items do not obscure important information—in this case, the level indicator—needed to monitor effectiveness and accuracy of treatment modalities.
Consult staff with required skills and knowledge
Issue: This event clearly demonstrates the issues facing healthcare staff who are not knowledgeable about the types of home-infusion devices used in their community. In this case, it was the Leventon Dosi-Fuser. Once the patient arrived in the ED, nobody thought to call ambulatory oncology pharmacists, who frequently handle these devices.
Lesson learned: Develop the expectation that expert(s) (those most familiar with the device) will be consulted when issues are suspected. When feasible, educate staff about the most common devices used in the community setting. For example, if the Leventon Dosi-Fuser is commonly used in the community to deliver home-based chemotherapy, then both ED staff and oncology staff should have basic familiarity with the device.
Conclusion
Since the error reported by the patient in this case turned out to be a false alarm, actions taken by the healthcare practitioners in response to the reported error resulted in an adverse outcome for the patient—the premature disconnection of the Dosi-Fuser and interruption of the full course of therapy. The patient never received the full dose of fluorouracil for that cycle, and the impact this may have on the overall treatment outcome remains unknown. Had a more thorough investigation been conducted when the patient first presented to the ED, a lot of anxiety, medical care, and resources could have been spared, and the adverse outcome could have been avoided.