
Problems Persist with Life-Threatening Tubing Misconnections
In our June 12, 2003 newsletter, we reported several cases in which the tubing from a portable blood pressure monitoring device was inadvertently connected to the patient’s IV line – in one case, leading to a fatal air embolism. In our September 4, 2003 issue, we wrote about an inadvertent connection of an air supply hose from a sequential compression device (SCD), also referred to as intermittent pneumatic compression, to a needleless IV tubing port. In that case, the SCD was turned off and the misconnection was found before any harm occurred.
Sadly, we recently learned about another tragic error involving the connection of oxygen tubing to a pediatric patient’s IV line. The child had been receiving medication via a nebulizer to treat asthma.
While still attached to a wall outlet, the oxygen tubing (AIRLIFE, from Allegiance Healthcare Corporation) became disconnected from the nebulizer fluid chamber (see Figure 1).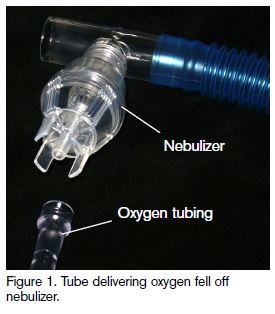 Later, a staff member accidentally reconnected the oxygen tubing to the injection port on a Baxter CLEARLINK Needleless Access System IV tubing Y-site.
Later, a staff member accidentally reconnected the oxygen tubing to the injection port on a Baxter CLEARLINK Needleless Access System IV tubing Y-site.
While oxygen tubing does not have a Luer connector, Baxter’s investigation into this event confirmed that such a connection is possible with their Clearlink valve (with oxygen tubing encompassing the Y site), albeit with excessive force (see Figure 2).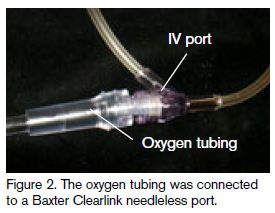
According to the FDA report on this event, the oxygen tubing disconnected from the IV tubing in seconds, but not before the pressure of the compressed oxygen supply forced the needleless valve open and allowed air into the tubing. The child died instantly. Baxter has since issued a safety alert advising of this hazard. However, the May 13, 2004, alert was sent only to directors of nursing, so others who need to know, including respiratory therapists, may have missed it.
Although these types of misconnections might be uncommon, the risk of a similar tragic event persists and is likely to be present in most hospitals – including yours! Baxter is exploring modifications to the Clearlink valve to prevent the potential for a recurrence elsewhere. Allegiance has also redesigned the specific oxygen tube to nebulizer connection with hard plastic to reduce separation. Still, we tested a variety of additional needleless devices that also accommodated oxygen tube connectors. Right now, oxygen tubing could very well connect to your needleless or standard IV tubing, including systems from Alaris, Baxter, B. Braun, BMP, Inc., Catheter Innovations, Clave, and Hospira (formerly Abbott). Clearlink is a clear needleless system, similar to some oxygen tubing, but the color on other needleless systems may not be a deterrent. Additionally, all medical gases and most fluids are clear, making it virtually impossible to distinguish between them when observed through transparent medical tubing. As in this case, many medical tubing “attachment” sites look quite similar, further increasing the risk of an error. With typical oxygen flow rates in liters per minute, a fatal pneumatic misconnection would require only seconds.
The best solution lies with eliminating interconnectivity between various medical tubings. The Association for the Advancement of Medical Instrumentation (AAMI) offers a publication (HE-74, Human factors design process for medical devices) that provides human factors engineering guidance to aid in the proactive testing of tubing interconnectivity in realistic settings. However, we are unaware of any specific domestic or international standards organization looking at mandatory standards for connector designs.
Take the time to review the medical equipment used in your facility to identify the potential for misconnections to IV tubing. Educate all staff, including non-clinical employees who work in patient care units, about this hazard, perhaps using storyboards to communicate the point effectively. Before tubing is connected or reconnected to a patient, require staff to completely trace it from the patient to the point of origin for verification. Appropriately labeled IV lines could help alert staff if they are about to access that line accidentally.
Also identify all types of staff in your organization who might connect, disconnect, or reconnect various forms of tubing (including IV tubing) attached to patients (e.g., technicians who work in diagnostic units, transport staff, nursing assistants, students, physicians), and consider whether this task falls within a safe and acceptable scope of practice. Certainly, trained licensed practitioners can inadvertently connect the wrong tubing to an IV line. However, untrained staff (e.g., ancillary personnel, medical and nursing students) are less likely to know and follow safety measures (such as tracing the line from the patient to the point of origin), or to be knowledgeable about the serious ramifications of misconnections. In fact, many unlicensed, untrained staff may disconnect or reconnect various tubing, or be asked inappropriately to perform specific tasks such as turning off pumps or pressing the PCA button before patient transport. Include prohibitions for these tasks during orientation, and when possible, offer new ancillary staff practice in turning down requests to connect or disconnect medical tubing.