
Multifactorial Causes of Tacrolimus Errors: Confusion with Strength/ Formulation, Look-alike Names, Preparation Errors, and More
A recent string of errors associated with tacrolimus, an immunosuppressant used primarily to prevent rejection in transplant recipients, prompted ISMP to review the literature and analyze related events reported to the US Food and Drug Administration (FDA) Adverse Event Reporting System (FAERS) and the ISMP National Medication Errors Reporting Program (ISMP MERP). We found that tacrolimus has been involved in many reported errors during the past decade that have been caused by a wide variety of factors, the most common of which are described below.
Tacrolimus Availability
Tacrolimus is commercially available for oral use in the US in 0.5 mg, 1 mg, and 5 mg capsules (immediate-release PROGRAF and generics, extended-release ASTAGRAF XL), and 0.75 mg, 1 mg, and 4 mg tablets (extended-release ENVARSUS XR). The drug is also available in 5 mg/mL, 1 mL ampuls (Prograf) for IV use after dilution only in patients who are unable to take oral medications, as anaphylactoid reactions have been reported with IV administration. Sublingual administration (off-label) of the immediate-release formulation (at approximately 50% of the oral dose) is suggested in some drug references (e.g., Lexicomp) for patients unable to take oral medications. If an oral liquid formulation is needed, it must be compounded.
Types and Causes of Errors
Drug strengths that differ by a factor of 10. Mix-ups between drug strengths that differ by a factor of 10 are a common type of dosing error among products available in 10-fold increments (e.g., ARIPiprazole, 2 mg and 20 mg; warfarin 1 mg and 10 mg; predniSONE 5 mg and 50 mg; buprenorphine 75 mcg and 750 mcg; EPINEPHrine 0.1 mg/mL and 1 mg/mL). So, it is not surprising that a number of mix-ups have been reported between the 0.5 mg and 5 mg strengths of tacrolimus. Most of the reported errors involved dispensing and administration of the 5 mg strength instead of the 0.5 mg strength. These may have been precipitated by the unsafe practice of not including a leading zero (i.e., .5 mg) when prescribing or displaying the 0.5 mg strength.
Some of the errors resulted in patient harm. For example, a nephrologist treating a patient who had been hospitalized with an elevated serum creatinine after a kidney transplant reported that the cause of the acute kidney injury was a tacrolimus overdose. The overdose was caused by a dispensing error in which the 5 mg capsules were provided instead of the 0.5 mg capsules. The patient had been taking 5 mg twice daily (10 mg) instead of 0.5 mg twice daily (1 mg) for approximately 1 month before hospitalization.
Various release formulations. Mix-ups between regular-release and extended-release tacrolimus formulations were another frequently observed theme during our review, again reflecting a common error type among the many drugs available in both conventional (immediate-release, regular-release) and modified (e.g., delayed-release, extended-release) formulations.
ADVAGRAF, an extended-release tacrolimus product marketed outside of the US by Astellas but later approved in the US under the trade name Astagraf XL, was the drug most frequently involved in mix-ups with regular-release tacrolimus. More than 60 reports of errors with this drug were submitted to FDA by the manufacturer (FDA receives both foreign and domestic reports from manufacturers). Leading up to the approval of Astagraf XL in the US, the manufacturer and FDA carefully assessed the error experiences with Advagraf to develop labeling and naming strategies to help mitigate confusion. For example, XL was added to the trade name Astagraf in the US to help draw attention to its extended-release formulation.
However, we can still learn from these cases and others, as the way tacrolimus appeared on electronic prescribing system screens frequently contributed to these errors, as it often does in the US. In one case, a physician mistakenly ordered “tacrolimus MR 0.5 mg capsules” when he intended to select “tacrolimus 0.5 mg” on the screen (“MR” means modified-release). When drugs are listed by their generic names, and different formulations exist, the eyes typically capture the name of the drug first, and then may miss any evidence that one may be selecting the wrong formulation.
Look-alike medication names. ISMP has documented more than 800 confused drug name pairs that have been published in our newsletters. One name pair that we have recently been asked to consider including on our list of confused drug names is tacrolimus and tamsulosin, an alpha1 blocker used to treat benign prostatic hyperplasia (and off-label to treat bladder outlet obstruction symptoms and distal ureteral calculi expulsion). Although the available strengths differ, we discovered that several mix-ups between tacrolimus 0.5 mg and tamsulosin 0.4 mg have been reported, some leading to patient harm.
For example, a liver transplant coordinator reported two incidences where outpatient pharmacies had dispensed tamsulosin 0.4 mg to patients who had been prescribed tacrolimus 0.5 mg. Tragically, both reported cases were believed to have contributed to the rejection of the transplanted liver. In another case, a patient had been hospitalized with symptoms of organ transplant rejection. During collection of a home medication list, a nurse noticed that the capsules in the patient’s vial of medication labeled as tacrolimus 0.5 mg were quite different in color than she expected. She contacted a pharmacist, who identified the capsules as tamsulosin 0.4 mg.
Confusion among brand names has been reported less frequently. In one case, it was discovered that a patient with a high tacrolimus serum level had been given Prograf 5 mg capsules, intended for another family member, instead of his prescribed PROSCAR (finasteride) 5 mg. Apparently, the Prograf had been placed in the patient’s dosing pill box by a family member in error instead of Proscar. Fortunately, the patient’s creatinine remained stable and he was not harmed by the error.
Confusion when dispensing more than one strength for the patient’s dose. With variable tacrolimus dosing based on the patient’s weight, type of organ transplant, response to therapy, adjuvant immunosuppressants, and other factors, any of the available capsule or tablet strengths might be needed to fill a prescription. However, the pharmacy may not stock all strengths, and/or several strengths of the drug may be needed to accommodate the patient’s total daily dose. This can lead to dosing confusion, particularly during the dispensing and administration phases of the medication-use process.
For example, dispensing errors have involved a mismatch between the total prescribed dose and the capsule or tablet strengths dispensed to provide each dose. In one case, the prescriber ordered tacrolimus 5 mg orally every 12 hours (10 mg daily). However, the pharmacy only stocked the 0.5 mg strength and a limited supply of the 1 mg strength. The prescription was mistakenly filled with the 0.5 mg capsules, with directions to take 2 capsules by mouth every 12 hours, along with 1 mg capsules, with directions to take 3 capsules by mouth every 12 hours. This resulted in the patient receiving only 8 mg of the drug daily.
Patient confusion is also a concern when various strength capsules or tablets are dispensed. For example, a post renal transplant patient was prescribed tacrolimus 6 mg orally every 12 hours. The initial prescription was partially filled with 1 mg capsules, with directions to take 6 capsules for each dose every 12 hours, until a supply of 5 mg capsules could be ordered to lower the cost of the prescription medication. Once the 5 mg capsules arrived in the pharmacy, the remainder of the prescription was filled using 5 mg capsules along with 1 mg capsules to achieve each 6 mg dose. A pharmacist had placed a note on the bag containing the medication in the will-call area as a reminder to talk to the patient about the change in capsule strength and the new directions for use. However, the note was not noticed, and patient counseling never occurred.
Although new directions had been provided on the labels of the two newly dispensed vials, the patient combined all the capsules into the initial prescription vial. The patient then took 6 capsules in the morning and 6 at night, as indicated on the label instructions. A month later, a very high serum tacrolimus level was obtained. Inspection of the patient’s supply of tacrolimus showed the two strengths commingled in the vial, with the 1 mg capsules predominantly on the bottom (meaning the patient took mostly the 5 mg capsules each day, up to 60 mg daily).
Manufacturer label confusion. One of the extended-release formulations of tacrolimus, Astagraf XL, comes in a bottle with a label that has occasionally confused patients who were dispensed the product in the sealed manufacturer’s (Astellas Pharma US) container. In one case, a patient who was previously taking immediate-release tacrolimus 3 mg every 12 hours had just been converted to 6 mg of the extended-release product Astagraf XL daily. The new prescription for Astagraf XL had been filled using sealed manufacturers’ bottles of the 1 mg capsules, onto which pharmacy labels had been applied, directing the patient to take 6 capsules daily. However, 1 week later, lab work showed that the tacrolimus trough had dropped to an undetectable level. 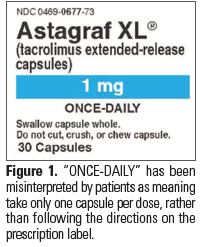 The patient had been taking only 1 mg of the drug daily, not the 6 mg dose. Instead of following the correct directions on the pharmacy label, the patient had been following what she thought were directions for use on the manufacturer’s label that stated, “ONCE-DAILY,” listed right below the drug name and dose (Figure 1).
The patient had been taking only 1 mg of the drug daily, not the 6 mg dose. Instead of following the correct directions on the pharmacy label, the patient had been following what she thought were directions for use on the manufacturer’s label that stated, “ONCE-DAILY,” listed right below the drug name and dose (Figure 1).
Compounding errors. Errors during the compounding of tacrolimus oral liquid formulations were also reported, including 10-fold overdoses and underdoses when the incorrect capsule strength was used for preparation (i.e., 0.5 mg instead of 5 mg), inappropriate substitution of a generic product for a brand name product, incorrect preparation of the suspension, and incorrect storage conditions. In two of the cases, a tacrolimus suspension was created using the wrong suspending agent. Tacrolimus is poorly soluble in water, so it is recommended to compound an oral suspension using Ora-Plus and Simple Syrup.1 Ora-Plus contains suspending agents, which prevent drug particles from aggregating and settling. This allows for the creation of a homogenous suspension and uniform concentration. One of the patients who received an incorrectly compounded suspension for which Ora-Plus was not used experienced problems with extreme fluctuations in his tacrolimus levels. The outcome for the second patient is unknown.
Safe Practice Recommendations
Standardize compounding concentrations and recipes. If oral liquid formulations of tacrolimus must be compounded, establish a standard concentration for pediatrics and adults, and provide staff with clear recipes that include the oral suspension vehicle (e.g., Ora-Plus and Simple Syrup, not water) to use along with detailed directions for preparing the suspension. A Michigan statewide initiative has created recipes with standardized concentrations for pediatric oral compounded liquids.2 These recipes, including one for tacrolimus, are freely available here. They include directions for preparation, data on stability, and storage information. The American Society of Health-System Pharmacists is also currently working on a project to provide standardized concentrations for intravenous and oral liquid medications.
Avoid leading decimal point doses. Always include a leading zero when expressing tacrolimus doses less than 1 mg on computer screens, device screens, pharmacy labels, shelf markers, and other paper and electronic formats. Whenever possible, avoid fraction doses greater than 1 mg by rounding the dose to the nearest whole number.
Monitor patients frequently. Tacrolimus has a narrow therapeutic index, so trough levels should be obtained for monitoring to prevent organ rejection (from levels that are subtherapeutic) and nephrotoxicity (from supratherapeutic levels).
Use brand names. Display the brand name of tacrolimus extended-release formulations (i.e., Astagraf XL, Envarsus XR) on drug ordering and verification screens to help differentiate these formulations from regular-release tacrolimus (i.e., Prograf, generics). When prescribing regular-release tacrolimus, use only the brand or generic name, without any modifiers such as “IR” for immediate-release.
Add to look-alike list. Consider including tacrolimus and tamsulosin on your organization’s look-alike drug name list, and increase the situational awareness of staff regarding the risk of potential mix-ups. (The drug name pair will be added to ISMP’s List of Confused Drug Names with the next update.)
Stock needed strengths. Stock all available strengths of tacrolimus that might be prescribed in your facility, and use the simplest single strength or combination of strengths to match the patient’s prescribed dose when dispensing the product.
Educate prior to discharge. Educate patients regarding the directions for taking the correct dose of tacrolimus, how to manage dose changes, and the importance of monitoring drug levels. Ensure that patients can repeat back the specific directions for taking each prescribed dose. Provide patients with information about the common types of errors that may happen with tacrolimus and how to prevent and detect these errors.
Conduct outpatient counseling. Establish a fail-safe mechanism to ensure that patients are counseled when picking up prescriptions for tacrolimus, particularly for the first prescription and whenever the dose, dosage strength, or formulation are changed.
Recommendations for FDA and drug companies. We call upon FDA and drug companies to avoid the availability of doses in 10-fold increments whenever possible. We also call upon the manufacturer of Astagraf XL (Astellas) and FDA to evaluate whether labeling changes are necessary given consumer confusion with the term “ONCE-DAILY.”
ISMP thanks Staley Lawes, PharmD, BCPS, FISMP, for her contribution to this article.
References
- Han J, Beeton A, Long PF, Wong I, Tuleu C. Physical and microbiological stability of an extemporaneous tacrolimus suspension for paediatric use. J Clin Pharm Ther. 2006;31(2):167-72.
- Michigan Pediatric Safety Collaboration. Tacrolimus suspension. Michigan Collaborative Standardization of Compounded Oral Liquids. April 2014.