
Administering Just the Diluent or One of Two Vaccine Components Leaves Patients Unprotected
When lyophilized (powdered) medications are co-packaged with manufacturer-supplied diluents, a danger exists that only the diluent will be dispensed and administered by practitioners who mistakenly believe it is the actual medication. This has been a recurring problem with various medications—glucagon, DOCEtaxel, and melphalan injections, for example. Another serious risk exists with two-component vaccines and vaccines that are packaged with a specific liquid component to be used as a diluent. If these vaccines are not prepared and administered properly, an individual could be unnecessarily exposed to serious and sometimes fatal communicable diseases, such as meningitis, pertussis, and others. Even worse, individuals may not know they are vulnerable to a disease if an error goes unrecognized or unreported.
Errors of this type are reported frequently. They account for 6% of all error types reported to the ISMP National Vaccine Errors Reporting Program, which began in late 2012. There are currently 12 vaccines that come with specific diluents and 2 vaccines provided with two-component containers that must be mixed prior to administering the dose. Reported errors with these vaccines frequently involve multiple patients. Typically, a practitioner dispensing or administering the vaccine fails to notice that a single dose requires combining the contents of two vials. Many times, these vials look very similar and may both emphasize the name of the active drug.
In the ISMP VERP database, we have seen reports in which:
- The practitioner dispensed or administered just the manufacturer-supplied diluent, or the practitioner reconstituted a lyophilized vaccine using an unintended diluent (e.g., sterile water, diluent from a different vaccine product) instead of the specific diluent provided. These errors were reported most frequently with the ActHIB [Haemophilus b conjugate] vaccine, which comes with a vial of 0.4% sodium chloride, provided by the manufacturer, to be used as a diluent.
- The practitioner dispensed or administered the contents of only one component (1 vial) of a two-component (2 vials) vaccine. These errors were reported most frequently with MENVEO (meningococcal [groups A, C, Y, W-135] diphtheria conjugate) and PENTACEL (diphtheria and tetanus toxoids, acellular pertussis adsorbed, inactivated poliovirus and Haemophilus b conjugate [DTaP-IPV/Hib]).
Specific examples of these errors follow.
Menveo
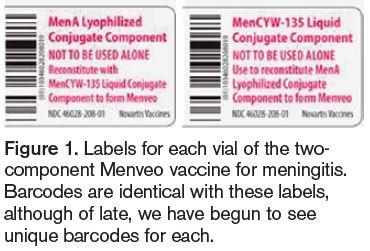 There were 14 reports submitted to the ISMP VERP involving the administration of only the liquid component of Menveo without the lyophilized powder component. Menveo induces immunity against meningococcal disease caused by Neisseria meningitidis serogroups A, C, Y, and W-135. It comes as a two-component vaccine supplied in 2 vials, one containing MenA powder and one containing MenCYW-135 liquid (Figure 1). The vaccine comes in a multidose carton containing 5 doses (10 vials total). A warning to administer both vials of vaccine is only visible on the back panel of the carton (Figure 2),
There were 14 reports submitted to the ISMP VERP involving the administration of only the liquid component of Menveo without the lyophilized powder component. Menveo induces immunity against meningococcal disease caused by Neisseria meningitidis serogroups A, C, Y, and W-135. It comes as a two-component vaccine supplied in 2 vials, one containing MenA powder and one containing MenCYW-135 liquid (Figure 1). The vaccine comes in a multidose carton containing 5 doses (10 vials total). A warning to administer both vials of vaccine is only visible on the back panel of the carton (Figure 2), 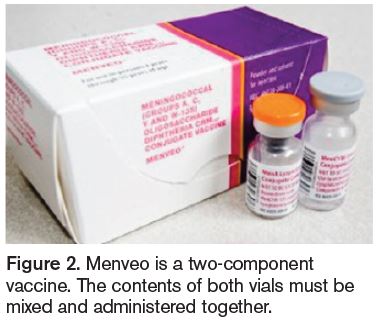 despite plenty of white space elsewhere. The warning states, “Neither MenCYW-135 nor MenA component to be used alone.” While the vial labels also contain language noting their proper use, one’s eyes are not immediately drawn to the warning to combine these products because it is presented in the same color font as the vaccine names (Figure 1). While the vials are slightly different sizes and have different cap colors, similarity in label style and color, and the small font size increase the risk of mistaking either vial as the complete vaccine.
despite plenty of white space elsewhere. The warning states, “Neither MenCYW-135 nor MenA component to be used alone.” While the vial labels also contain language noting their proper use, one’s eyes are not immediately drawn to the warning to combine these products because it is presented in the same color font as the vaccine names (Figure 1). While the vials are slightly different sizes and have different cap colors, similarity in label style and color, and the small font size increase the risk of mistaking either vial as the complete vaccine.
Several errors also suggest that practitioners may mistakenly believe the “liquid” component of the vaccine is just a standard diluent. As such, some errors involved administration of only the MenA powder after it was reconstituted with a “generic” diluent (e.g., sterile water) or diluent supplied with other vaccines (e.g., varicella, MMR). In addition, some of the errors in which the liquid MenCYW-135 component was given alone were reported as administration of just a “diluent,” without recognition that the “liquid” component is part of the vaccine. In a recent report, the barcodes on the MenA and MenCYW-135 vials were identical (Figure 1). However, DailyMed now provides examples of the vial labels with unique barcodes; thus, a bedside bar-coding system could help catch an error if only one vial was being used.
Pentacel
There were also 14 reports involving Pentacel (Figure 3), a two-component vaccine for active immunization 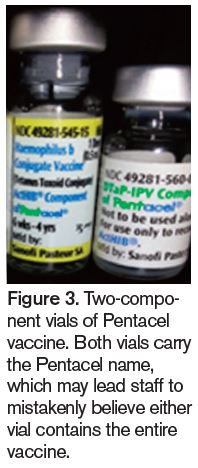 against diphtheria, tetanus, pertussis, poliomyelitis, and invasive disease due to Haemophilus influenza type b. The vaccine is available in a 5-dose carton containing vials of DTaP-IPV liquid component (with blue caps), which are used to reconstitute vials of the lyophilized ActHIB component (with green caps). Ten of the reports involved infants who had to return to their providers to receive just the inadvertently omitted ActHIB component. Four of the 14 cases involved reconstitution of the ActHIB powder with a sterile diluent intended to reconstitute other vaccines (e.g., varicella, MMR). In these cases, the patient did not receive the DTaP-IPV component of the vaccine. Both of the vials carry the Pentacel name, so a practitioner unfamiliar with this two- component vaccine might believe that either vial, or the one carrying the Pentacel name at the top of the label, is all that is needed for vaccination.
against diphtheria, tetanus, pertussis, poliomyelitis, and invasive disease due to Haemophilus influenza type b. The vaccine is available in a 5-dose carton containing vials of DTaP-IPV liquid component (with blue caps), which are used to reconstitute vials of the lyophilized ActHIB component (with green caps). Ten of the reports involved infants who had to return to their providers to receive just the inadvertently omitted ActHIB component. Four of the 14 cases involved reconstitution of the ActHIB powder with a sterile diluent intended to reconstitute other vaccines (e.g., varicella, MMR). In these cases, the patient did not receive the DTaP-IPV component of the vaccine. Both of the vials carry the Pentacel name, so a practitioner unfamiliar with this two- component vaccine might believe that either vial, or the one carrying the Pentacel name at the top of the label, is all that is needed for vaccination.
ActHIB
Four errors involved the ActHIB vaccine, which is a lyophilized powder that comes with a diluent. The outer carton back panel notes that it contains 5 single-dose vials of vaccine and 5 vials of saline diluent. Also on the back panel in very small print is a notation to reconstitute the vaccine with the diluent provided. The vaccine and diluent vial labels are both yellow with black print. The label on the diluent states, “Diluent for Haemophilus b conjugate vaccine.” However, if it is not known that the vaccine is provided with its own diluent, it would be easy to reconstitute the powder with a “generic” diluent, which is what happened in all 4 reported cases. Also, if the diluent alone is picked up, it could be mistaken as the vaccine if the term “Diluent” is overlooked.
Other products
The other vaccines with at least one error of this type reported to the ISMP VERP included the M-M-R II (measles, mumps, rubella) vaccine, PROQUAD (measles, mumps, rubella, varicella virus) vaccine, and oral ROTARIX (rotavirus) vaccine. Most of these errors involved administering just the diluent or diluting the vaccine with the wrong diluent. Errors with oral Rotarix vaccine and its special diluent were described in our February 13, 2014, newsletter.
Error detection and reporting
We suspect that many errors with these types of vaccines remain undetected or are not reported. The ISMP VERP program is only 1½ years old and is still not widely known. Yet, 40 reports of errors involving two-component vaccines and lyophilized vaccines packaged together with diluents have already been received. Errors that have been reported were mostly detected by chance when a nurse or pharmacist was checking vaccine stock and noticed that there were extra or missing vials of one of the two-vial vaccine pairs. For example, many of the Menveo errors were detected when a nurse or pharmacist noticed extra vials of the powdered form of the vaccine but fewer vials of the liquid component. Follow up then determined that an error had occurred.
Patient impact
If numerous patients received an improperly prepared vaccine before an error was noticed, many reporting practitioners felt they could not be certain which patients received an incomplete vaccination. Thus, revaccination attempts may have overlooked some patients who received just part of the vaccine. Even when casting the net wide to identify all potentially affected patients, practitioners reported that some patients declined to return for revaccination. Thus, some patients remain unprotected due to these errors.
Vaccine labeling recommendations
With the recent trend in delaying or skipping vaccinations due to uninformed vaccine safety messages in the media, it is critical to make sure those who do choose to become vaccinated or to vaccinate their children receive safe and effective vaccines. ISMP believes vaccine manufacturers must do more to improve vial labeling to reduce the risk of errors with these crucial products, especially the two-vial vaccines. This specific problem has been longstanding, and the interim measures taken to date are not keeping patients safe. The labeling on vaccines and diluents or two-component vaccines must clearly distinguish each vial, yet connect the two products so their contents are administered together. This is no easy task, but it is one that manufacturers should undertake. Suggestions for consideration include:
- Label the vials as Vial 1 of 2 and Vial 2 of 2, or use a similar scheme to distinguish yet link the 2 vials whose contents must be administered together.
- Provide clear directions for use and warnings to administer the contents of both vials together on the front carton label and vials—perhaps on their caps.
- Make any warnings stand out on the label by employing text in colors that differ from the standard text on the label. (Consider the problem with Menveo labels [Figure 1] where all text is the same reddish color.)
- Conduct usability testing with vaccine users to test labels for clarity and effectiveness. Look for ways that the vial labels can be misunderstood and whether anticipated changes might improve understanding. Design labels to reduce the risk that either vial is mistaken as the complete vaccine alone.
- Ensure there are unique NDC numbers and barcodes on each vaccine component and diluent.
Vaccine packaging recommendations
- Barring stability or similar issues, vaccine manufacturers should determine whether they can package two-component vaccines and diluents in new and novel ways to promote safety. Suggestions for consideration include:
- When product stability and storage allow, package the vaccines in dual-chamber syringes (Figure 4)
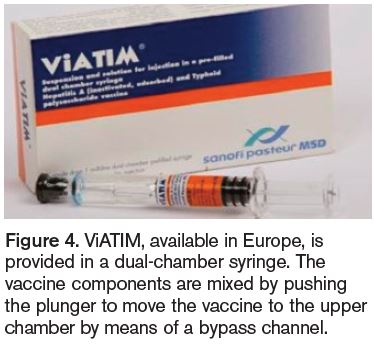 similar to a European vaccine product, VIATIM (hepatitis A and typhoid polysaccharide vaccine), from Sanofi Pasteur MSD). While the initial cost of the product may be higher, the need for revaccination in the event of an error would likely negate any cost increase. An additional advantage includes a single expiration date for both products. (Currently, each vial’s expiration date may be different.)
similar to a European vaccine product, VIATIM (hepatitis A and typhoid polysaccharide vaccine), from Sanofi Pasteur MSD). While the initial cost of the product may be higher, the need for revaccination in the event of an error would likely negate any cost increase. An additional advantage includes a single expiration date for both products. (Currently, each vial’s expiration date may be different.) - Package the vaccines in dual-compartment containers similar to SOLU-MEDROL (methylPREDNISolone sodium succinate) (Figure 5). This packaging (or the dual-chamber syringes) would keep the 2 components or vaccines and diluents together and help ensure that the correct components are administered together.
- Package the vaccines in redesigned vials that accommodate larger labels to reduce label crowding.
- Attach or connect the 2 vials in a way that facilitates selection of both vials at the same time but allows separation if necessary to prepare the vaccine for administration.

Vaccine practice recommendations
- Establish ongoing education of staff (e.g., nurses, pharmacists, medical assistants) who may dispense and administer vaccines. Include discussion of safety issues with two-component vaccines and vaccines packaged with specific diluents. Be sure staff understand the differences between two-component vaccines and vaccines packaged with specific diluents.
- Distinguish the most critical information on vaccine containers by circling the information, highlighting the information, or using auxiliary flag-type labels without obscuring existing label information.
- If using a vaccine that requires a specific diluent for reconstitution or two components that must be combined before administration, if stability allows, keep the two vials together using a rubber band or place them together in a sealable plastic bag. Light-protected bags are available for purchase. Affix an auxiliary label to the vaccine to remind staff to use both vials.
- Label the areas where vaccines are stored to facilitate correct selection and to remind staff to combine the contents of vials. Examples of vaccine labels for storage areas are provided by the Centers for Disease Control and Prevention).
- To confirm administration of both vaccine components, document the NDC number for each vial in the vaccine log before administration. Documenting actual administration of the vaccine should always occur after it is given, which can also provide an opportunity for a double check.
Conclusion
For years, ISMP has contacted vaccine manufacturers to suggest enhanced labels and packages, and we have repeatedly covered vaccine safety in our national advocacy efforts, publications, and educational programs. Thanks to the ISMP VERP and the many healthcare practitioners who have taken the time to report vaccine errors to the program, we are now better equipped to identify trends affecting vaccine safety and provide more detailed analysis of the causes and prevention of vaccine errors. We hope to build on the relationships we have established in the vaccine community to identify the best practices for both practitioners and vaccine manufacturers. If you have any suggestions regarding vaccine safety, please contact us.